Two new studies underscore the superiority of PET/CT for imaging lung lesions compared to either modality alone. One group of researchers presenting at the 2005 European Congress of Radiology (ECR) in Vienna found that different fusion methods produced substantially different results.
Hardware-based CT fusion was more accurate than standalone software in a presurgical lung cancer staging study, according to Dr. Benjamin Halpern from the University of California, Los Angeles and the University of Vienna. A second paper from Leuven, Belgium, found that PET/CT had higher sensitivity, specificity, and positive and negative predictive values than either modality alone for detecting lung metastases.
Better staging with dedicated PET/CT
"Previous studies have suggested improved staging accuracy for lung cancer with hardware fusion," Halpern said at an ECR chest tumor session. "And software fusion is considered an inexpensive alternative to hardware fusion as seen by the group in Zurich" (New England Journal of Medicine, June 2003, Vol. 348:25, pp. 2500-7000).
The Swiss group relied on hardware-based fusion with their dedicated PET/CT scanner. So far, however, no clinically validated study had compared the performance of hardware and software fusion, Halpern said. The UCLA team took on this task, retrospectively comparing the accuracy of PET, hardware fusion, and software fusion in a well-defined population of 36 patients with non-small cell lung cancer (NSCLC).
"The patient population consisted of 19 female and 17 male patients with mean age of 68 years," Halpern said. "The most frequent underlying lung cancer types were pure adenocarcinomas with 18 cases, followed by adenocarcinomas with mixed cellularity and squamous cell carcinomas."
Within 16 days before surgery or mediastinoscopy, all patients underwent imaging on a dedicated Reveal RT PET/CT (CPS Innovations, a joint venture of Erlangen, Germany-based Siemens Medical Solutions and CTI Molecular Imaging of Knoxville, TN). Single-modality PET images were acquired on a Topaz PET scanner, and the imaging exams were followed by mediastinal node dissection.
Additionally, 25/36 (69%) patients had a separate noncontrast lung CT study within six weeks of hardware PET/CT scan, and these images were used to perform software-based fusion on commercially available software (Mirada Solutions, Oxford, U.K.).
"The software fusion is divided up into two sections, first the rigid transformation, which is limited to translation, rotating, and scaling," Halpern said. "This is followed by deformable transformation, which allows for correction of the (image) integration, like breathing or movement of internal organs. No manual alignment of PET/CT was done before the fusion."
The PET images were interpreted by consensus of two nuclear medicine physicians; a radiologist joined them in the interpretation of hardware, software, and fusion images. The images were scored as positive or negative for disease, and staged according TNM tumor classifications.
In all, 30/36 patients had T-stage assessment. PET alone correctly staged 20/30 (67%) patients, compared to 29/30 (97%) patients at PET/CT, a statistically significant difference (p < 0.05). In three cases PET underestimated tumor size, and in three cases the tumors were FDG-negative, Halpern said.
In N staging as well, PET/CT tended to be more accurate than PET alone (78% versus 69%). Hardware-based PET/CT correctly staged 25/30 (83%), and PET understaged nine patients compared to PET/CT, which overstaged one.
"The reasons for N understaging were -- both for PET and PET/CT in three cases -- subcentimeter lymph nodes, in two cases an incorrect assignment of node station with PET, and in just one case with PET/CT," Halpern said. "Both PET and PET/CT overstaged three cases due to granulomatous disease, and one case due to anthracosis. In two cases PET suspected disease, but no disease could be found by histopathology to correlate with CT."
Software fusion's advantages were less clear. The fusion process was successful in 17/25 (68%) patients, but failed in eight (32%) cases. In all successful cases, the same T and M stage could be achieved as with hardware fusion, Halpern said.
"However, when measuring all three dimensions, the misalignment was considered to be higher for software fusion, 15.4 cubic mm, compared to 7.2 cubic mm for hardware fusion," he said.
The results showed that hardware-based PET/CT fusion staged NSCLC more accurately than PET, Halpern concluded. But, he emphasized, PET/CT's superior diagnostic performance was limited to T staging, and no significant difference could be seen in N staging. Software fusion failed in 32% of the cases, but when successful it produced the same results as hardware fusion, he said.
Not the software's fault
The reason for hardware-based PET/CT's superiority may be as simple as the acquisition protocol, Halpern said in response to a question from session co-moderator Dr. Fergus Gleeson from Oxford University in the U.K. Gleeson had asked Halpern why he thought software fusion performed so poorly.
Unlike hardware-based PET/CT, Halpern responded, the acquisition protocols are different when the images are acquired separately, and include shallow breathing rather than a breath-hold in the PET exam. With two acquisition protocols "you get a completely different volume of oxygen in lungs -- and virtually no software fusion program is capable of fusing images that are from different breathing protocols," Halpern said.
Even when fusion fails, the images can still be fused manually, Halpern said, though at five minutes per image the process is time-consuming. PET and CT can also be read side by side, of course.
PET/CT better for lung metastases
In the next presentation at the ECR session, Dr. Walter De Wever from University Hospitals Gasthuisberg in Leuven, Belgium, discussed his group's study of patients with suspected lung metastases by PET and PET/CT.
"We examined 34 patients with a known primary tumor, and all these patients underwent PET/CT for the staging of tumor. We detected 56 lung metastases, and the clinical diagnosis was based on the anatomical or virtual exam, or on follow up (for) at least six months," De Wever said.
CT was evaluated by a radiologist, who was joined for the hardware-integrated PET/CT images by another reader, a radiologist and nuclear medicine specialist. They looked for lung nodules, and were asked to determine whether or not the lesions were metastatic, rendering the results by consensus.
 |
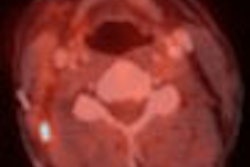
| A 55-year-old man with colorectal carcinoma. Patient underwent a PET/CT examination for tumor staging. CT showed a nodular lesion in the left lower lobe suspect for lung metastasis. PET examination could not reveal a suspected hot spot, but when the PET-CT correlation images were evaluated, a subtle hot spot was detected at the place of the lung nodule, which confirmed the metastatic origin of this nodule. Images courtesy of Dr. Walter De Wever. |
The results for specificity, sensitivity, positive predictive value (PPV), negative predictive value (NPV), and accuracy are shown below for each modality:
|
For the detection of lung metastases, PET alone is a little better CT, but PET/CT is more accurate than either modality, De Wever said.
 |
| A 48-year-old man with lymphoma. Patient underwent a PET/CT examination for follow-up. CT of the chest was normal. PET examination revealed a hot spot in the right upper lung region that was suspect for lung metastasis. PET-CT showed that this lesion was a bone metastasis, not a lung metastasis. Images courtesy of Dr. Walter De Wever. |
"When we use a CT method to detect lung metastases, we detect a lot of small nodules due to high spatial resolution, and characterization is based on morphological evaluation by size, by evaluation of margins, and by internal characteristics such as the constitution and uptake of contrast, and by evaluation of doubling time," he said. So CT is more suggestive of metastases than really diagnostic.
PET, of course, yields findings based on increased metabolism in the mucosa, and has a high negative predictive value, De Wever said. But PET can fail to detect lesions smaller than 1 cm, as well as lesions with low glucose avidity. PET findings can be difficult to localize. And combining the two modalities presents technical challenges, including motion and respiratory artifacts, he said.
By Eric Barnes
AuntMinnie.com staff writer
April 26, 2005
CT, PET staging may negate need for mediastinoscopy in lung cancer, April 11, 2005
FDG-PET/CT tops other technologies for lymphoma staging, March 23, 2005
PET/CT planning allows for greater gamble on NSCLC radiotherapy, March 16, 2005
PET/CT demonstrates staging strength over PET, CT, and PET plus CT, March 7, 2005
Copyright © 2005 AuntMinnie.com