CT's role in penetrating trauma evaluation has grown rapidly with improving technology. For many such injuries, MDCT is less invasive and more sensitive than the alternatives. Sensitivity concerns remain in a couple of applications, but it's hard to beat CT's unique advantages, including the ability to follow a gunshot wound track to the focus of an organ injury.
"To even talk about using CT scans to evaluate people with penetrating trauma 10 years ago would have been nothing short of heresy," said Dr. Amy Sisley, a trauma physician and assistant professor of surgery at the University of Maryland in Baltimore. "It really is a challenge to the old golden rule that the only safe way to evaluate penetrating trauma is with a knife."
Sisley discussed the spectrum of penetrating injuries, and weighed the alternatives for exploring them in a recent talk at the Society of Critical Care Medicine (SCCM) meeting in San Francisco.
Part of CT's growing role in penetrating trauma can be attributed to the trend toward nonoperative management. In areas plagued by high rates of violence -- stab wounds and shootings had reached crisis levels in cities like Durbin in South Africa and Medellin in Columbia -- nonoperative management was the only way to handle the enormous patient loads, Sisley said. Resources were simply not available to perform exploratory laparotomies on all those patients.
"In addition, I think we've all come to recognize the cost and morbidity of the so-called nontherapeutic exploration," Sisley said. The need has dovetailed with improving technology in the form of more detector rows and thin-section imaging as well as 3D software, giving CT an overall boost.
In penetrating extremity trauma, the classic indications for immediate exploration, including hemodynamic instability, pulsatile hematoma, significant hemorrhage, and limb ischemia, still apply, Sisley noted. Arteriography remains the imaging gold standard because it is extremely accurate, with a false-negative rate of less than 1% and a false-positive rate of about 2.5%.
However, she noted, a 1989 study showed that the ankle-brachial index (ABI) could be used to determine if a patient actually needed arteriography. In turn, trauma physicians were happy to find out they could sometimes avoid invasive and time-consuming arteriography with its incidence of complications such as vessel thrombosis, intimal dissection, groin hematoma, arterial spasm leading to ischemia, and distal embolization of atheromatous plaques.
On the other hand, CT arteriography can be completed in a few minutes, though it requires careful coordination of the acquisition with high-flow contrast media administration. And in the course of a few minutes, 3D reconstructions can enable the clinician to view the vasculature from every angle.
Most important, CT may be as accurate as arteriography, Sisley said, citing a head-to-head study by Busquets et al, who assessed the performance of CT arteriography in 95 patients who had undergone arteriography.
The authors found that "CTA adequately demonstrated the nature and location of all the arterial injuries when compared with conventional arteriography or surgical exploration." CTA found 21 arterial occlusions, two intimal flap defects, and two pseudoaneurysms. Nine of the 25 injuries were confirmed by surgery only, 10 by surgery and arteriography, and six by arteriography alone. CT had no false negatives (Journal of Trauma, March 2004, Vol. 56:3, pp. 625-628).
Transmediastinal injuries, usually from gunshot wounds, are of particular concern due to the risk of vascular, esophageal, and trachobronchial injuries, she said. The traditional workup is expensive and time-consuming, encompassing angiography to identify major blood vessels, bronchoscopy, esophagoscopy to look for trachobrochial injuries, and then a pericardial window to assess the heart -- or cardiac ultrasound, which is a very sensitive indicator of pericardial fluid. But there's a better way, she said.
First, chest x-rays would be obtained for the FAST exam to look for pericardial fluid. Then spiral CT of the chest would direct further evaluation. Only if the patient had a potential trachobronchial injury identified on chest CT would bronchoscopy be performed. A major advantage of CT in penetrating injuries is its ability to depict the missile tract, she said.
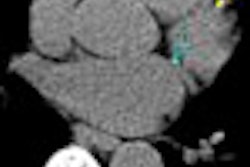
"The trajectory of the bullet can be followed if you use thick cuts on the CT scan, because it always leaves a little air path behind it that in many instance will guide you right to the injury -- so you can tell if the bullet is passed near certain structures or through certain structures," Sisley said.
 |
| CT shows bullet tract outlined by shrapnel on gunshot wound to the right side of the abdomen. Image courtesy of Dr. Amy Sisley. |
A study by Stassen et al examined the medical records of 22 transmediastinal gunshot wound patients, finding seven with positive CT scans. Directed further diagnostic evaluation of these patients revealed two who required operative intervention, and the remaining 68% with negative scans had no further treatment. CT did not miss any injuries compared with other diagnostic exams, and thus provides a safe, effective, and lower-cost method of examining such patients, they authors concluded (Journal of Trauma, October 2002, Vol. 53:4, pp. 635-638).
Penetrating abdominal wounds
Mandatory exploratory laparatomy is the traditional method of dealing with penetrating abdominal wounds, but "our thinking has changed" in recent years, Sisley said, with the understanding that morbidity associated with exploratory laparatomy is not insignificant. Complications rates for negative laparatomy range from 20% to 40%, she said.
Laparatomy is still an urgent need in the setting of hemodynamic instability or clinical signs of peritonitis, she said. When this is not the case there all alternatives, though none are optimal.
Serial abdominal exams, for example, are unreliable and labor-intensive. They cannot be done if the patient is in shock or unconscious, and from a practical standpoint it's impossible to have the same physician examine the patient every eight hours for 24 hours.
Local wound exploration is another option, aimed at determining if the peritoneal cavity has been penetrated. Often there is no injury that needs to be repaired, however, so this method produces a significant number of negative or nontherapeutic laparotomies.
Diagnostic peritoneal lavage (DPL) is hampered by a lack of consensus on what constitutes a positive confirmation of major intraperitoneal hemorrhage. A positive test based on a red blood cell count of greater than 100,000 per cubic millimeter will result in too many missed injuries, while a standard of greater than 5,000/mL or higher will produce too many negative laparotomies, she said. On the other hand, CT can be a useful tool when used optimally.
"What we're really interested in is CT's ability to predict the need for laparatomy, not just the need for peritoneal penetration," she said.
CT is quite sensitive to the presence of free peritoneal air, which would not be present in blunt trauma, but air can be misleading because the clinician can't tell if it entered through the wound shaft, or is associated with the injury. As a result, small amounts of free air are not a reliable indicator of injury. On the other hand, Sisley said, oral contrast is absolutely essential.
"If it leaks, that gives you a pretty good idea that there's a hole in the bowel," she said. "And with penetrating trauma, that's what you're really concerned about."
How good is CT for determining if the peritoneum has been penetrated? Sisley's University of Maryland colleagues Shanmuganathan et al examined 200 patients prospectively using triple-contrast spiral CT. CT had 97% sensitivity (66 of 68 findings), 98% specificity (130 of 132 findings), and 98% accuracy (196 of 200 findings) for peritoneal violation.
"The most sensitive CT finding of bowel injury was a wound track that extended up to the injured bowel, which was seen in 77% of patients (20 of 26)," the authors wrote. "It is important to know the precise wound entry site(s) and number of wounds and to employ optimal CT window and level settings (window width, 550 HU; level, 75 HU) to accurately identify wound tracks" (Radiology, June 2004, Vol. 231:3, pp. 775-784).
Two patients had false-negative CT findings for peritoneal violation. Both were stabbed in the left thoracoabdominal region and underwent therapeutic laparatomy. One patient had thickening of the left side of the diaphragm and a small left-sided hemothorax, the authors noted.
Diaphragm injuries are difficult to diagnose, Sisley said, and there really isn't a good test for them, though exploratory laparatomy or laparoscopy can do the job. Recently CT has been making advances in finding diaphragm injuries, which occur in 18% to 24% of penetrating abdominal trauma cases. Here again the way to find them on CT is to follow the wound track and see if it goes near the diaphragm, she said.
"In other words, if you see injury to the liver, then you see the diaphragm interposed, and then you see injury to the other side of the liver. It's a pretty good bet that the diaphragm went through the liver," she said. A discontinuous diaphragm or thickening of the diaphragm can also be an indication of injury.
In a study of patients known to have peritoneal penetration, CT predicted whether laparatomy was needed in 71 of 75 (95%) patients (Journal of Trauma, November 2001, Vol. 51:5, pp. 860-868).
CT hasn't traditionally been considered the modality of choice for bowel injuries but it is improving, and in the bowel, contrast extravasation is again the easiest way to determine if there's a problem, Sisley said.
"CT in penetrating trauma really has an emerging role," she concluded. "Part of that is driven by the new technology of CT, which has improved tremendously its ability to detect injuries. It's noninvasive. And at the present time the big concern is false negatives, especially involving bowel and diaphragm -- that's a bigger concern than false positives."
By Eric Barnes
AuntMinnie.com staff writer
February 20, 2006
Related Reading
CT is the blanket modality for neuroimaging blunt injury patients, January 12, 2006
MDCT spurs boom in ER CT utilization, January 4, 2006
When x-ray finds cervical spine injuries, CT picks up more, September 14, 2005
CT procedure volume surges, February 4, 2005
CT: An all-star modality for C-spine trauma? August 18, 2004
Copyright © 2006 AuntMinnie.com