Most nongenital cancers that spread to the ovaries originate in the gastrointestinal tract. Making the distinction between primary and metastatic ovarian tumors is essential for proper patient care, according to a study in the September issue of the American Journal of Roentgenology.
Dr. Hyuck Jae Choi and colleagues used CT to document the differences between ovarian metastasis that spreads from either stomach cancer or colon cancer. Choi's group is from the National Cancer Center in Koyang, South Korea.
"Misinterpretation of a metastatic ovarian tumor as a primary tumor may have adverse consequences for the patient, such as unnecessary surgery or inappropriate chemotherapy or radiation therapy," they wrote. "The results of our study strongly suggest that specific CT findings are useful for differentiation ..." (AJR, September 2006, Vol. 187:3, pp. 741-745).
For this retrospective study, the patient population consisted of eight out of nine women with 13 ovarian metastatic lesions from stomach cancer and 23 out of 27 women with 31 ovarian lesions from colon cancer. They all underwent contrast-enhanced CT on a four-slice scanner (Mx 8000, Philips Medical Systems, Andover, MA). The scanning protocol was a detector array of 4 x 1.25 mm, beam pitch of 1.35, section thickness of 3.2 mm, and 3-mm reconstruction.
 |
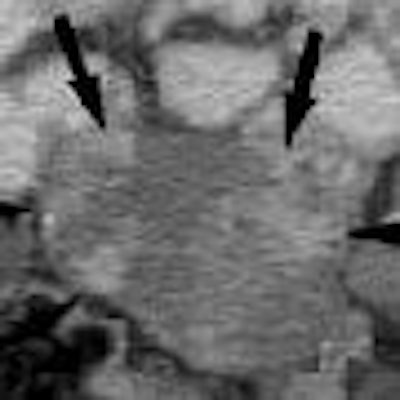
| A 60-year-old woman with unilateral ovarian metastasis from stomach cancer. Contrast-enhanced CT scan showed mainly solid, oval, moderately enhancing mass with smooth margin in left adnexa. Dense enhancing portions (arrows) are evident in mass. Choi HJ, Lee JH, Kang S, Seo SS, Choi JL, Lee S, Park SY, "Contrast-Enhanced CT for Differentiation of Ovarian Metastasis from Gastrointestinal Tract Cancer: Stomach Cancer vs. Colon Cancer" (AJR 2006; 187:741-745). |
The CT images were read in consensus by two radiologists who recorded multiple ovarian mass characteristics including laterality, size, margin, shape, and enhancement. Based on histopathology, the majority of the ovarian lesions that metastasized from stomach cancer were signet-ring cell carcinoma (76.9%). The majority of the lesions that metastasized from colon cancer were tubular adenocarcinoma (61.3%).
According to the imaging findings, ovarian metastatic lesions from stomach cancer were more solid than those from colon cancer, with more prominent enhancement but more discrete enhancement patterns. Ovarian masses from colon cancer tended to be larger, possibly because they are more cystic in nature, the authors stated.
Also, the colon cancer patients with ovarian metastasis were generally older. "Specifically, 37.5% (3/8) of the patients with ovarian metastasis from stomach cancer were younger than 40 years, whereas none of the patients in the other group were younger than 40 years," the authors wrote. This might be attributed to the increase in the number of younger patients with stomach cancer, which is a more aggressive disease in this patient group, they added.
Using the CT imaging characteristics, "we accurately differentiated the origin of ovarian metastasis in (72.7%) of 44 cases.... Our CT results showed that mass characteristics, laterality, enhancement of the solid portion, and size are valuable parameters," the authors concluded.
The group acknowledged that they worked with a small sample size and that a certain selection bias may have occurred because cases of primary ovarian cancer were not included. However, they noted that one of the main jobs of the radiologist in this setting was to be able to discern between primary and secondary neoplasms.
By Shalmali Pal
AuntMinnie.com staff writer
August 23, 2006
Related Reading
Extracolonic findings double VC costs, but might be worth paying, July 20, 2006
IL-18 and FGF-2 complement CA125 in detecting ovarian cancer, May 12, 2006
US, CT show similar strengths in pelvic pain imaging, May 3, 2006
Copyright © 2006 AuntMinnie.com