The use of primary 3D interpretation isn't generally recommended for reading reduced-prep virtual colonoscopy (VC) data. Reading is time-consuming, and the monochromatic lumps and bumps typically rendered in 3D endoluminal views can make it difficult to distinguish polyps from residual stool.
But a new study says that reading reduced-prep data in 3D is not only possible but accurate and time-efficient if a software translucency rendering tool is applied, and iodinated oral contrast is administered to do part of the job of a traditional prep.
In general, 3D endoluminal viewing "better depicts haustral folds, increases polyp conspicuity, and is more intuitive for radiologists with limited training," said principal investigator Dr. Antonio Guerrisi from the University of Rome "La Sapienza."
In addition, primary 3D interpretation of VC data "has been validated for colon cancer screening using a Viatronix workstation" (New England Journal of Medicine, December 4, 2003, Vol. 349:23, pp. 2191-2120), he noted. "However, 3D viewing has two major disadvantages: it increases the number of false-positive lesions and has longer interpretation times."
One possible way to reduce false positives and negatives in 3D is translucency rendering (TR) -- software that color maps minor differences in attenuation. Different colors (blue, green, red, and white) are assigned to areas of increasing attenuation, making it easier to distinguish the relatively homogeneous density of true polyps from more heterogeneous residual materials.
But although TR is considered invaluable for prospective screening at primary 3D reading, it has not been proven effective by statistical analysis, Guerrisi said.
"3D translucency rendering is an accurate tool to easily differentiate true polyps from polypoid-like fecal residues during real-time 3D fly-through," he said. "However, unmarked fecal residues (FP calls) or opacified-coated true polyps (FN calls) may still be misinterpreted," necessitating the use of 2D confirmation in all cases. "So the purpose of the study was to evaluate the efficacy of translucency rendering for differentiating polyps from polyp-like residues," he said.
The retrospective study, presented at the 2007 European Congress of Radiology (ECR) in Vienna, included 50 pathologically proven polyps and 50 polypoid-like fecal residues, all from patients who underwent VC (or CT colonography [CTC]) without cathartic preparation.
Fecal tagging was achieved using diatrizoate meglumine and diatrizoate sodium (Gastrografin, Schering, Berlin), which has a mild cathartic effect. Over two days each subject ingested 200 mL total of the agent (20 mL x five meals), and followed mild dietary restrictions that proscribed fibrous foods.
Following automated colonic insufflation with CO2 (ProtoCO2l, E-Z-EM, Lake Success, NY), the researchers acquired low-dose CT images using a 64-slice scanner (Sensation 64, Siemens Medical Solutions, Erlangen, Germany) set at 0.6 x 64-mm collimation, 3-mm slice thickness, 140 kVp, and 10 mAs.
Three experienced radiologists who had completed more than 200 VC exams each examined the data independently using a primary 3D technique, and dedicated software (V3D Colon, Viatronix, Stony Brook, NY) equipped with translucency rendering.
Based on the color pattern generated by translucency rendering for each lesion, readers were asked to assign a diagnostic confidence level using a four-point grade scale (1 = definitely fecal residue, 2 = probably fecal residue, 3 = probably polyp, 4 = definitely polyp).
Polyp detection was high with 49, 48, and 48 of 50 lesions correctly characterized by readers 1, 2, and 3, respectively (average specificity for polyp characterization, 96.6%). With regard to polypoid fecal residues, 48, 47, and 48 lesions were correctly characterized by readers 1, 2, and 3, respectively (average specificity for fecal residue characterization, 95.3%).
 |
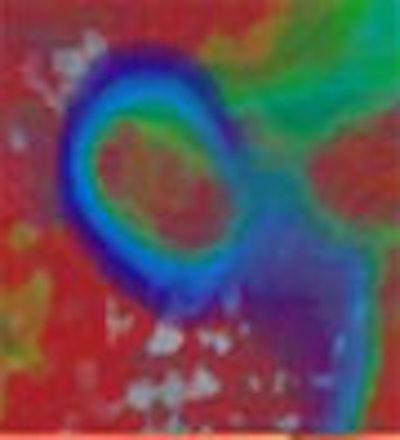
| Above, concentric circles and homogeneous interior of lesion depict the presence of a true polyp on translucency rendering software (Viatronix V3D Colon), shown with adjacent 2D correlations. Below, heterogeneous density of polypoid findings help identify residual fecal material. All images courtesy of Dr. Antonio Guerrisi. |
 |
"TR is an adequate tool to easily differentiate true polyps from polypoid-like fecal residue during real-time 3D interpretation," Guerrisi concluded. "However, polyps can be misinterpreted." Larger, prospective studies are needed to confirm the tool's effectiveness, he added.
From the audience, Dr. Anno Graser from the University of Munich in Germany said that TR was certainly a time-saver, but less helpful for distinguishing polyp morphology.
"I've been using this tool and I think it is useful," Graser said. "But my experience is that if you have a lesion of intermediate density -- one where you really aren't sure -- this is where translucency rendering will not have an answer for you either." So while TR saves time, it does not help distinguish polyps from residual material, he said.
"TR is not magic, it simply avoids some of the time-consuming 2D correlations," commented Dr. Perry Pickhardt from the University of Wisconsin in Madison, who uses TR software in daily practice.
"All soft-tissue lesions require 2D correlation," Pickhardt wrote in an e-mail to AuntMinnie.com. "TR increases 3D specificity but not does improve overall specificity of CTC (i.e., it makes the 3D display more powerful, but the underlying truth always resides in the indispensable 2D images). Just because 2D is poor for finding polyps (sensitivity) that doesn't take away from its ability distinguish true from false lesions (specificity)."
As for primary 3D reading of prepless virtual colonoscopy data, he added: "I think the Italians are on the right track with diatrizoate (Gastrografin), as opposed to barium, which by itself is unsatisfactory," Pickhardt said. "I feel that (Gastrografin and barium) are synergistic and best used in tandem."
By Eric Barnes
AuntMinnie.com staff writer
May 14, 2007
Related Reading
Screening model calls VC most cost-effective colon exam, April 24, 2007
Group favors 3-D primary read in major virtual colonoscopy trial, September 2, 2003
New data reveal higher efficacy for primary VC screening, October 18, 2006
Virtual colonoscopy: 2-D vs. 3-D primary read, June 3, 2002
Copyright © 2007 AuntMinnie.com


















