Virtual colonoscopy (VC or CT colonography) is a promising way to sort through patients with a positive fecal occult blood test (FOBT), considering the latter's demonstrated low sensitivity and high false-positive rate. Or so it would seem.
But in a screening cohort from the Netherlands, polyps and cancer were so common in FOBT patients that VC hardly seemed worth it. Had the group been screened with VC in a clinical setting, at least half would have needed subsequent optical colonoscopy and polypectomy.
"FOBT is a simple and cheap test for screening for colorectal cancer in a screening population," said Dr. Marjolein Liedenbaum from the Academic Medical Center and University of Amsterdam in the Netherlands. "It is known that FOBT can reduce mortality from colorectal carcinoma by 17%. However, the test generates lots of false positives. Therefore, it might be possible to use [CT colonography (CTC)] in an FOBT-positive population; then colonoscopies could be reduced."
The study of 150 FOBT-positive screening patients, half of the cohort of 300 that will eventually participate, aimed to determine VC's accuracy in this population. Liedenbaum presented the preliminary results at the 2008 European Congress of Radiology (ECR).
Two types of FOBT tests were used on the population: guaiac FOBT tests (n = 32) and immunochemical FOBT tests (OC-Sensor, Eiken Chemical, Tokyo) (n = 118).
Previous studies have shown a 5% to 12% sensitivity for colorectal cancer with guaiac-based FOBT and a positive predictive value for adenomas of about 33%, Liedenbaum said. The immunochemical test has higher reported sensitivities -- about 6% for small adenomas, 35% for advanced neoplasia, and 65% for invasive cancers.
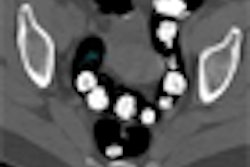
All subjects underwent a three-day noncathartic bowel prep consisting of ingestion of an oral iodinated contrast agent (7 mL Telebrix, Guerbet, Roissy, France) in conjunction with a low-fiber diet. Following CO2 insufflation of the bowel with a rectal catheter, a low-dose imaging protocol was performed prone and supine on a 64-detector-row CT scanner.
"Two expert readers experienced in CTC interpretation reviewed all of the data, and a double-reading was performed," Liedenbaum said. "The results of both readers were added and no consensus was done."
Segmentally unblinded virtual colonoscopy served as the reference standard for the study. A research fellow matched colonoscopy-detected lesions to VC-detected lesions by size and location.
Seven percent (n = 11) of the FOBT-positive patients had colorectal carcinomas, all of which were identified at CTC and subsequently at optical colonoscopy. Among the FOBT-positive subjects, 49% had large lesions (10 mm or larger) and 73% had medium-sized lesions (6 mm or larger).
VC's per-patient sensitivity was 96% and 93% for large and medium-sized polyps, respectively. For the immunochemical (OC-Sensor) test, per-patient sensitivities were 96% and 94%, respectively, for large and medium-sized polyps, and for the guaiac FOBT test, 95% and 92%, respectively.
Per-patient specificity was 92% and 77% for large and medium-sized polyps, respectively (OC-Sensor: 91% and 82%, respectively; guaiac FOBT: 100% and 50%, respectively).
"CTC might be more effective in the OC-Sensor group than in the hemoccult FOBT-positive group because of [FOBT's] low specificity for lesions 6 mm and larger, but there was only a small number [n = 32] of patients with a hemoccult FOBT-positive test, so we will have to wait for the other half of the patients," she said. Even so, she added, specificity for this test should be well below 50%.
"We see that CTC shows a high diagnostic accuracy in the detection of colorectal carcinoma in polyps in patients who are FOBT-positive," Liedenbaum said. "However, CTC as a triage method is still questionable, because larger numbers of FOBT-positive patients than we expected had polyps 10 mm or larger and 6 mm or larger."
Dr. Anno Graser from the University of Munich in Germany said he was surprised to see a study so apparently at odds with the literature regarding FOBT's sensitivity, which was higher than previously reported, especially because adenomas do not commonly bleed to cause a positive FOBT exam.
Liedenbaum said it is too early to interpret the results at this point in the study, which could be due to a higher prevalence of adenomas in the Dutch population -- or the study population. And it will be helpful to see the results for the other 150 patients, she said.
By Eric Barnes
AuntMinnie.com staff writer
July 28, 2008
Related Reading
FOBT screening reduces emergency colorectal cancer admissions, March 25, 2008
Fecal occult blood screening reduces mortality rates, December 3, 2007
Testing for colorectal cancer on the rise, but barriers to screening still exist, March 17, 2008
American Cancer Society recognizes virtual colonoscopy screening benefit, March 5, 2008
Five-modality Munich trial finds high sensitivity for OC, VC, November 12, 2007
Copyright © 2008 AuntMinnie.com