Computer-aided detection (CAD) software can improve the detection of flat lesions at virtual colonoscopy (also known as CT colonography or CTC) -- as long as the lesions are at least 1 mm high. In a new study from Italy, CAD detected 94% of all flat lesions; however, radiologists dismissed a few of them incorrectly as false positives.
Researchers from the University of Rome "La Sapienza," led by Dr. Franco Iafrate, examined 31 patients with flat lesions who underwent both virtual and conventional colonoscopy as part of a larger study.
"We know that with flat lesions, those reported to be < 3 mm in elevation or more than three times larger than their height, there has been some controversy regarding the prevalence and clinically optimal screening methods," Iafrate said at the 2009 European Congress of Radiology (ECR) in Vienna. "We know that CTC can detect flat lesions of the colon; however, flat lesions can be potentially difficult to detect when there is only 1-2 mm elevation."
Missed flat lesions are often attributed to inadequate distention, spatial resolution, or inadequate cleansing, he said. And although CAD has been shown to help increase detection sensitivity for polyps 6 mm and larger, its sensitivity for detecting both flat and diminutive colorectal lesions needs to be looked at more carefully.
"The purpose of our study was to evaluate the ability of CAD software to evaluate morphologically flat lesions at CTC," he said. In order to do that, two expert radiologists -- working in consensus and fully unaware of the endoscopic results -- read the images without and then with the aid of CAD" (CAD-COLON v. 1.10, Im3D, Turin, Italy), he said.
The 31 cases included 15 patients undergoing surveillance after polypectomy, five with a positive family history of colorectal polyps or cancer, and 11 average-risk screening subjects. Nearly all (n = 28) subjects skipped a full bowel prep in favor of a low-fiber diet with the addition of fecal and fluid tagging (150 mL gastrografin) the day before the exam, while the remaining three subjects underwent a full cathartic bowel preparation.
After insufflation of the colonic lumen with room air, prone and supine scans were acquired using a 64-detector-row LightSpeed VCT scanner (GE Healthcare, Chalfont St. Giles, U.K.) at 1-mm collimation and 50 mAs. After the virtual colonoscopy exam, all subjects underwent conventional colonoscopy and histological assessment of any lesions removed at polypectomy.
"We performed the exams normally using 2D and 3D for problem-solving, then applied the CAD, which presented a number of possible lesions" for acceptance or rejection by the radiologists, Iafrate said.
The researchers also logged reading times with and without CAD, the number of false positives on supine and prone, and sensitivity vis-à-vis conventional colonoscopy, he said. The combined results revealed 34 endoscopically proven lesions defined as flat, including:
- 19 lesions 3 mm in height
- 11 lesions 1-2 mm in height
- 2 lesions < 1 mm in height
- 2 lesions three times diameter versus height
There were four flat lesions in the transverse colon, 13 in the ascending colon, 11 in the cecum, four in the descending colon, and two in the rectum, Iafrate said. Visualized flat lesions were 3 mm or less in height and 6 mm or greater in diameter.
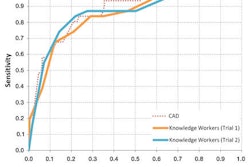
- 26 of 34 (76%) flat lesions were detected by the radiologists alone
- 32 of 34 (94%) flat lesions were detected by CAD alone
- 30 of 34 (88%) lesions were detected by CAD plus the radiologist
 |
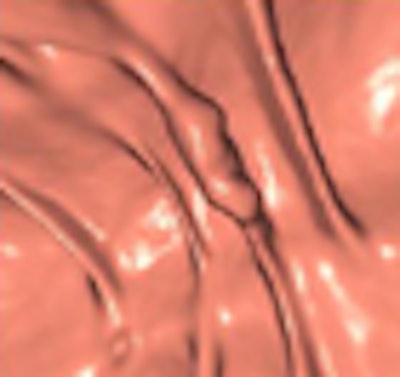
| Two low-grade dysplastic polyps < 1 mm in height, including a "carpet" lesion, were not detected by CAD or initially at CTC (left, middle), but were later found at CTC and conventional colonoscopy (right). All images courtesy of Dr. Franco Iafrate. |
At histology, 22 of 34 (65%) had low-grade dysplasia, he said. No colorectal cancers were found. Two cigar-shaped true-positive lesions detected by CAD were dismissed by the radiologists due to low conspicuity.
 |
| Two true-positive lesions detected by CAD were dismissed by radiologists due to low conspicuity and a "cigarlike" appearance; both were also detected at conventional colonoscopy. |
"Six lesions located on the haustral folds showed a much higher conspicuity on the 3D endoluminal views than on 2D," he said. For polyps on folds, focal thickening and surface nodularity were key features leading to their detection.
 |
| Six lesions detected at CAD and VC on haustral folds were more conspicuous in 3D endoluminal views (right) than on 2D (left) visualization. Key features included focal fold thickening and surface nodularity. |
Two lesions < 1 mm in height were not detected by either CAD or the radiologists, but were found at conventional colonoscopy. Both could be seen retrospectively at CTC as a focal wall thickening.
Mean reading time for 2D plus 3D problem-solving was 4 minutes and 28 seconds, with CAD analysis adding a mean 52 seconds, he said.
"Twenty-five percent of lesions were missed without CAD, and CAD improved lesion detection from 75% to 90%, so we can conclude that CT colonography can detect flat lesions in the colon," Iafrate said.
"However, flat polyps can be difficult to detect when there is only 1 mm elevation," he said, adding that many of these patients have other lesions higher than 1 mm, increasing the likelihood that even these will be found at CTC. "CAD improves flat lesion detection," he said.
In response to a question from the audience, Iafrate said the readers knew beforehand that they would be looking for flat lesions, but added that he did not believe the knowledge affected their reading sensitivity.
By Eric Barnes
AuntMinnie.com staff writer
June 6, 2009
Related Reading
VC's high positive predictive value important for colonoscopy follow-up, April 30, 2009
Adding CAD to virtual colonoscopy saves lives and money, February 24, 2009
Minimal-prep VC may miss more flat lesions, April 17, 2008
CAD nabs the flat polyps VC readers may miss, March 9, 2008
Flat colorectal tumors relatively common in U.S. population, linked to cancer, March 5, 2007
Copyright © 2009 AuntMinnie.com