Dutch researchers are taking computer-aided detection (CAD) of the lungs beyond suspicious lung nodules and into the diagnosis of chronic obstructive pulmonary disease (COPD), aiming to identify the patients most likely to benefit from treatment.
"The mortality, morbidity, and treatment costs of COPD are increasing. COPD is expected to be the third cause of death by 2020," said Bram van Ginneken, PhD, an associate professor of radiology at Radboud University Nijmegen in the Netherlands.
COPD is unique in that it involves at least two disease processes, which vary in combination, presentation, and severity from patient to patient, van Ginneken said in a presentation at the 2010 Computer Assisted Radiology and Surgery (CARS) meeting in Geneva.
"A lot of people think there's not just one type of COPD but different types, and these processes have different contributions, which might actually be the reason why a lot of trials for drugs for COPD have failed -- because they take all COPD patients instead of finding a subgroup in which the drug might work," van Ginneken said.
COPD includes a small-airway disease component in the form of inflammation that can be seen indirectly at CT. The small airways themselves are not visible, he said, but small, collapsed airways can be seen as air trapping on expiration CT.
The second component is destruction of the parenchyma (characterized by loss of alveolar attachments and reduced elastic recall) that's also visible on CT as emphysema -- dark areas on the scans, van Ginneken said. The contribution of these two processes varies by patient.
Automated tools are a must for exploring both these disease processes; the measurements are far too complex to perform manually, van Ginneken said. The algorithms analyzing CT lung images will have to be robust and reliable to quantify disease components and determine the severity and contribution of each component, he said.
Fortunately, algorithms developed at van Ginneken's facility can do everything that's needed for analysis when they're used in combination, the study found.
Van Ginneken and colleagues analyzed 231 CT scans in patients for whom both an inspiratory and expiratory scan were available. They were equally distributed over the four Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages -- a lung function scale established to define COPD severity.
The GOLD classification system is based on lung function rather than disease etiology, as expressed in the standard spirometry measurement FEV1/FVC (the ratio of forced expiratory values [FEV] to forced vital capacity [FVC]). GOLD stage 0 is defined as the presence of symptoms of cough, sputum, and breathlessness without airflow obstruction. Stages1 to 4 are identified as follows:
- Stage 1: Reduced FEV1/FVC ratios less than 70% of predicted values, and reduced FEV1 versus predicted values of > 80%
- Stage 2: Reduced FEV1/FVC ratios of 50% to 80%
- Stage 3: Reduced FEV1/FVC ratios of 30% to 50%
- Stage 4: Reduced FEV1/FVC ratios of < 30% (patients with respiratory failure or cor pulmonale are deemed stage 4 regardless of their FEV1)
In their study, van Ginneken and colleagues examined their subjects with several tests on the same day, including:
- Low-dose CT at full inspiration (16 x 0.75 mm, 120-140 kVp, 30 mAs)
- Ultralow-dose CT at full expiration (16 x 0.75 mm, 90 kVp, 20 mAs)
- Pulmonary function testing
They used algorithms developed at the facility over the past few years for automated segmentation, including:
- Lungs (Van Rikxoort et al, Medical Physics, July 2009, Vol. 36:7, pp. 2934-2947)
- Lobes (Van Rikxoort et al, IEEE Transactions on Medical Imaging, June 2010, Vol. 29:6, pp. 1286-1296).
- Airways (Van Ginneken et al, MICCAI 2008)
"We autosegmented the lungs, the lung lobes, and the airways in those scans, and then we extracted the airways, which were excluded from further analysis," he said. Scans were acquired in pairs including low-dose inspiration and low-dose expiration, and if processing failed in one scan, the entire pair was also excluded from analysis. But there was very little failure.
"It turned out, actually, that in most of the pairs, we were able to correctly segment these structures automatically," he said.
After segmentation, lobar analysis was used to examine the data based on the following thresholds:
- Marker for emphysema: Percentage lobar volume in inspiration scan below -950 HU (IN-950)
- Marker for air trapping: Percentage lobar volume in expiration scan below -850 HU (EX-850)
- Normal values per lobe for IN-950 and EX-850 derived from GOLD stage 0 subjects
- Cutoffs per lobe: Values > mean + 2 standard deviation were classified as abnormal
"A well-known marker for emphysema is to look at how much of the lung volume in inspiration scans is below a certain threshold -- in this case, -950 HU for air trapping," van Ginneken said.
To analyze air trapping, they inspected the lobes in the expiration scan and computed the percentage of tissue below -850 HU. Normal values were based on those of GOLD stage 0 subjects in the database, i.e., patients without a clinical diagnosis of COPD. The mean value and standard deviation of the two markers were determined, with cutoff values based on the mean value plus two times the standard deviation.
Finally, each lobe was classified. If IN-950 was above the cutoff, the lobe was considered emphysematous; otherwise, if the lobe was too dark in expiration, it was classified as affected by air trapping, but otherwise normal.
 |
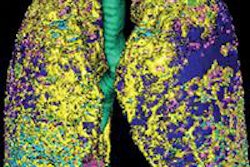
| Above, images from the inspiration scan of a 74-year-old man diagnosed as GOLD stage 3. There is emphysema (dark areas) throughout the lungs, and only the lower right lobe is not substantially affected. Below is the overlay image based on thresholding at -950 HU, including the percentages for each lobe as a whole. Four lobes, except the lower right, are above their cutoff values, meaning that this patient has an emphysema-dominant COPD phenotype. The right lower lobe was also not affected by air trapping. All images courtesy of Bram van Ginneken, MD, PhD. |
 |
 |
| Above, images from the expiration scan of a 65-year-old man with GOLD stage 3. The image shows increased density in some areas, common in expiration scans, but also regions that remain dark and are indicative of air trapping. Below, the overlay images from a single coronal section show that the left upper lobe is normal, while two lobes had emphysema and two had air trapping, indicating mixed-phenotype COPD. |
 |
 |
| As disease severity progresses from GOLD stage 0 to higher stages, the number of patients with four or all lobes within the normal range decreases, as expected. |
In the intermediate GOLD stages, the results showed a substantial subgroup of patients with mixed-phenotype and with predominantly small-airway disease.
"We hypothesize that this may be the group that responds to drug treatment," van Ginneken said. "But it you look at very severe COPD patients, they usually have all their lobes affected by emphysema."
Reliable CAD tools enable a very nuanced analysis of the pathology, he said. "But whether this is the right way to derive an imaging biomarker from CT scans, I think, is a very open research area," he said. "You could also look at the airways -- airway lumens and airway walls. We're looking at that, and other groups are looking at it as well."
By Eric Barnes
AuntMinnie.com staff writer
October 1, 2010
Related Reading
CAD detects signs of emphysema on DR images, September 27, 2010
Bundling of CAD software boosts lung lesion detection at CT, September 21, 2010
Combined PET/CT CAD improves lung nodule detection, August 6, 2010
CT method measures airway calcium to diagnose lung cancer, June 28, 2010
Altered blood flow in lungs predicts emphysema, April 6, 2010
Copyright © 2010 AuntMinnie.com