In a new study that used computer-aided analysis, the presence of low normal lung tissue volume correlated with pulmonary arterial hypertension at 3D CT. The technique could offer a more accessible and less invasive diagnostic test than right heart catheterization, according to researchers from Japan.
Looked at another way, in patients with chronic fibrosing interstitial pneumonia, low normal lung tissue volume is useful for predicting pulmonary hypertension, especially in individuals with coexisting emphysema, as often occurs in smokers, the study group found (American Journal of Roentgenology, August 2014, Vol. 203:2, pp. W166-173).
Low normal lung volumes at 3D CT negatively and significantly correlated with pulmonary hypertension in patients with chronic fibrosing interstitial pneumonia, the authors wrote. And at logistic regression analysis, a reduced percentage of normal lung tissue accurately predicted pulmonary arterial hypertension (PAH).
 Dr. Tae Iwasawa, PhD, from Kanagawa Cardiovascular and Respiratory Center.
Dr. Tae Iwasawa, PhD, from Kanagawa Cardiovascular and Respiratory Center.But there was only a weak correlation between mean pulmonary artery pressure and fibrosis, which might help explain previous studies in which the fibrosis score on CT images did not correlate with pulmonary hypertension. In these studies, the patients were mostly nonsmokers who did not also have emphysema, which together with fibrosis may contribute to PAH.
"The main finding of our study is that decreased normal lung volumes correlate with pulmonary hypertension in the patients with both emphysema and pulmonary fibrosis," lead author Dr. Tae Iwasawa, PhD, a radiologist from Kanagawa Cardiovascular and Respiratory Center, told AuntMinnie.com by email.
"Our results suggest that quantitative measurement of normal lung volume can be useful for predicting pulmonary hypertension in patients with chronic fibrosing interstitial pneumonia, especially those with coexisting emphysema," the authors wrote.
Fibrosis or emphysema?
PAH is a negative complication of idiopathic interstitial pneumonia (IIP), while idiopathic pulmonary fibrosis (IPF) is the most common form of chronic fibrosing interstitial pneumonia in IIP, the authors explained. The development of PAH in IIP patients has important prognostic implications -- leading to higher one-year mortality rates compared to patients with IIP but no PAH.
But there's a diagnostic problem: Overlapping symptoms of shortness of breath and exercise limitation make it difficult to detect hypertension in IIP patients. Right heart catheterization is the most accurate tool available, but it is invasive and expensive, spurring the need for a noninvasive alternative, the authors wrote.
In theory, fibrogenesis should correlate with pulmonary hypertension, but previous studies have not shown this correlation, probably due to the presence of emphysema, itself a well-known factor for pulmonary hypertension. In patients with lung damage caused by both fibrosis and emphysema, isolating the main contributor to pulmonary hypertension can be difficult, according to the authors.
"We hypothesized that normal lung volume correlates negatively with the severity of pulmonary hypertension," Iwasawa and colleagues wrote. "In many of the previous studies on this topic, the main target of CT evaluation in IIP was the extent of fibrosis; normal lung volume was not measured directly. In this study, we examined whether the CT-determined lesion volume data, especially normal lung, correlated with pulmonary hypertension in patients with IIP."
The retrospective study looked at 40 consecutive patients with IIP who underwent both right heart catheterization (RHC) and chest CT. The group included 33 (82.5%) smokers or former smokers. All had shown interstitial abnormalities suggestive of pulmonary fibrosis in the lower lung zones on CT images, and almost half (19/40) had undergone surgical lung biopsy and were also diagnosed histopathologically with pulmonary fibrosis.
Thin-section CT images were acquired during inspiration on a 64-detector-row scanner (Aquilion 64, Toshiba Medical Systems) without contrast, and right heart catheterization was performed a mean 31 days from the CT scan.
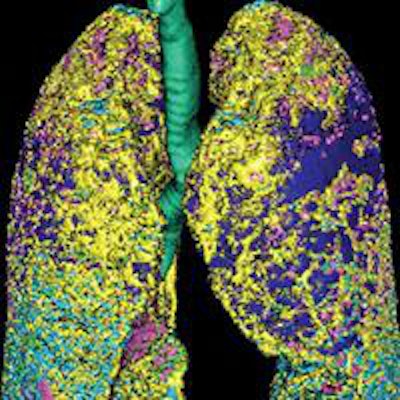
 Images are of a 69-year-old man with idiopathic pulmonary fibrosis and emphysema. The patient was a former smoker (45 pack-years). Mean pulmonary artery pressure was 29 mm Hg, measured by right heart catheterization. Above left, computer-aided analysis showed 32.5% emphysema, 16% fibrosis, and 35.7% normal lung tissue volume. Above right and below, sagittal reformatted CT images show computer-aided segmentation results corresponding to the top left image. Pink = normal, dark blue = emphysema, light green = ground-glass opacity, light blue and yellow = fibrosis, dark green = trachea and bronchi, and orange = vessels. Images republished with permission from the American Roentgen Ray Society.
Images are of a 69-year-old man with idiopathic pulmonary fibrosis and emphysema. The patient was a former smoker (45 pack-years). Mean pulmonary artery pressure was 29 mm Hg, measured by right heart catheterization. Above left, computer-aided analysis showed 32.5% emphysema, 16% fibrosis, and 35.7% normal lung tissue volume. Above right and below, sagittal reformatted CT images show computer-aided segmentation results corresponding to the top left image. Pink = normal, dark blue = emphysema, light green = ground-glass opacity, light blue and yellow = fibrosis, dark green = trachea and bronchi, and orange = vessels. Images republished with permission from the American Roentgen Ray Society.
The lung volumes were examined on a computer-aided system that used CT attenuation values to distinguish fibrotic from normal, consolidated, and emphysematous regions on a PC. The automated tool extracts the lung from the CT images using a semiautomated threshold technique. Next, the bronchial trees and blood vessels are removed.
The algorithm categorized the lungs pixel by pixel, and then calculated the relative volume of each lesion to the CT lung volume as "normal(%)," "ground-glass opacities(%)," "consolidation(%)," "emphysema(%)," and "fibrosis(%)."
Finally, logistic regression analysis was used to evaluate the relationship between each lung "volume(%)" and pulmonary hypertension, and receiver operator characteristics (ROC) curves were used to assess the predictive value of these CT-based volumes in identifying pulmonary hypertension.
The results showed that 16 of the 40 patients had pulmonary hypertension at rest (mean pulmonary artery pressure [PAP] > 25 mm Hg on RHC).
There were no significant differences between the pulmonary hypertension group and the nonhypertension group with regard to age, smoking habits, or time between CT and right heart catheterization. However, the median diffusing capacity was significantly worse in patients classified as positive for pulmonary hypertension, the authors wrote.
The median diameter of the pulmonary artery was larger (mean, 34.7 mm) in patients with PAH than in those without hypertension (mean, 30.6 mm).
At multivariate analysis of each volume(%), normal(%) was a significant predictor of pulmonary hypertension (odds ratio, 0.92; 95% confidence interval: 0.86-0.96; p = 0.02). On ROC analysis, the area under the curve of normal(%) was 0.849 (95% confidence interval: 0.731-0.967).
And although there were no significant differences between the groups in fibrosis or ground-glass opacity scores, the median total score was significantly greater in those with PAH than those without it (4.1 versus 3.1, respectively). Among the 40 patients, 13 had emphysema that occupied more than 10% of lung volume, but only eight of the 13 were classified as having pulmonary hypertension.
"In this study, normal lung volume, represented by normal(%) on 3D CT images, correlated negatively and significantly with pulmonary hypertension in patients with chronic fibrosing interstitial pneumonia," Iwasawa and colleagues wrote.
When analyzed using logistic regression analysis, decreased normal(%) of lung areas accurately predicted PAH, but there was a weak correlation between mean PAP and fibrosis(%), they wrote. Moreover, total lung volume measured at CT did not correlate with mean PAP -- which can be explained by the coexistence of emphysema.
"The noninvasive and accessible nature of CT makes it an attractive tool for predicting pulmonary hypertension," the authors wrote. "The pathobiology of pulmonary hypertension in pulmonary fibrosis is not completely understood. However, our results suggest that quantitative measurement of normal lung volume can be useful for predicting pulmonary hypertension in patients with chronic fibrosing interstitial pneumonia, especially those with coexisting emphysema."
There are important things to learn about these patients that the study doesn't address, Iwasawa pointed out in her email. "Low normal lung volume is an important finding, but heart disease and pulmonary arterial thromboembolism [PTE] are also important," she said. "Our study excluded patients with heart disease and PTE."
As for the automated lung volume analysis tool, it worked well but still needs fine-tuning. Outside of the study, "I don't use this technique routinely," she said.
"Our system needs some improvements in the man-machine interface," Iwasawa said. "Now we are seeking a company to commercialize it. I think quantitative analysis of CT is necessary for pulmonary fibrosis. I hope that our system will be used worldwide."


















