CHICAGO - Individualized contrast media protocols can cut the use of contrast and the radiation dose while optimizing contrast attenuation for suspected pulmonary embolism (PE), according to South Carolina researchers. The use of an automated algorithm to choose imaging parameters delivered reliable image contrast in all of the target vessels, they found.
The evolution of CT has markedly improved imaging to rule out PE in recent years, resulting in better spatial resolution, better contrast enhancement, and faster scan times. CT is now the reference standard for ruling out pulmonary embolism. Unfortunately, the development of scanning protocols hasn't kept pace with the development of the scanners themselves, said J. Michael Barraza in a presentation at the 2010 RSNA meeting. Use of an automated technique to minimize dose and contrast use while maximizing attenuation of the target vessels can help radiologists make better use of new CT scanning technologies, he said.
There are many different patient-, scanner-, and contrast-medium-specific factors that affect the timing of contrast enhancement, including cardiac output and body weight, scan duration and delay, and injection rate and duration, and concerns about radiation dose make it essential to optimize PE imaging protocols, said Barraza, who is from the Medical University of South Carolina (MUSC) at Charleston.
"Contrast-injection protocols have failed to evolve at the rate of scanners, preventing realization of their full diagnostic potential," Barraza said in his presentation. "Most CT angiography studies of the chest still use fixed injection protocols, or adjust the contrast volume to estimate the duration of the scan acquisition." The common result: Poor opacification of target vessels, higher-than-necessary radiation doses, and overuse of contrast, with artifacts that can mimic stenosis, he said.
The study evaluated the performance of a computerized algorithm (P3T, Medrad, Indianola, PA) to determine individualized, patient-based contrast media injection parameters for high-speed CT angiography (CTA) of the chest.
Researchers retrospectively examined 91 patients who underwent high-speed CTA of the chest using 128-detector-row dual-source CT (Somatom Definition Flash, Siemens Healthcare, Malvern, PA) in Flash mode. The indications for scanning included:
- CT pulmonary angiography (CTPA) in 34 patients
- Coronary CTA in 19 patients
- Triple rule out (TRO) in 38 patients
The contrast medium was administered using a dual-syringe injector (Stellant D, Medrad) based on patient weight, scan duration, contrast medium concentration, and the attributes of the timing bolus scan. The software calculates delay time, contrast volume, injection rate, and contrast and saline mixing ratios, as well as the total iodine dose and delivery rate "based on the relationship between patient weight and scan duration," Barraza explained.
The target attenuation was set at 300 HU or greater in the pulmonary arteries for CTPA and TRO protocols, 350 HU or greater in the coronary arteries, 200 HU or greater in the right ventricle for coronary CTA, and greater than 350 HU in the coronaries and aorta for TRO. An observer measured attenuation in each of the patient scans and compared it to the target attenuation, and also reported scan duration, dose-length product, and contrast dose.
"Every single image was considered diagnostic quality," Barraza said, and every measured region was well above the target attenuation for each indication.
- In CT pulmonary angiography studies, the mean attenuation in the central pulmonary arteries was 443 ± 129 HU.
- At coronary CTA, mean attenuation was 492 ± 156 HU in the coronary arteries, 445 ± 157 HU in the left ventricle, and 321 ± 168 HU in the right ventricle.
- In TRO studies, the mean attenuation was 403 ± 83 HU in the coronary arteries, 351 ± 77 HU in the pulmonary arteries, and 407 ± 81 HU in the descending aorta.
Additionally, the researchers found "no significant correlation between pulmonary artery attenuation and scan duration, contrast volume, or [body mass index (BMI)]," Barraza said. In the TRO studies, however, there was significant correlation between coronary artery attenuation and BMI -- the only significant correlation seen among the three protocols.
 |
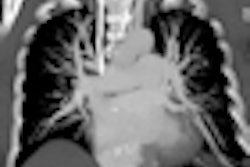
| Axial images of the thorax above and below were created from a pulmonary embolism study acquired in 0.2 seconds at dual-source CT in Flash mode, using the P3T algorithm to create the contrast injection protocol. The pulmonary and segmental arteries are well-enhanced (> 300 HU), with adequate enhancement in the aorta. The contrast protocol was created based on the patient's weight, scan duration, contrast concentration, and time to peak of a 15-mL timing bolus. This patient received 68 mL of 370 mgI/mL contrast at 5.2 mL per second. (A mixture phase of 35 mL, 20% contrast, was followed by a saline flush of 40 mL, all at the same flow rate.) Images courtesy of J. Michael Barraza. |
 |
The computerized contrast media delivery algorithm evaluated in this study consistently reaches or exceeds the desired vascular target attenuation at high-speed, low radiation-dose CTA of the chest, Barraza said. However, he added, the retrospective nature of the study is a central limitation. Prospective studies are needed to compare the diagnostic efficacy of this algorithm with those of standard injection protocols. In addition, the cohort was small, "however, additional studies are being analyzed that thus far demonstrate the same degree of high vascular attenuation," he said.
"The software facilitates seamless individualization of contrast injection for a variety of clinical circumstances, without compromising vascular attenuation," Barraza said. Application of the algorithm "can help ensure peak performance of current-generation CT scanners, preventing repeat scans and additional radiation exposure," he said. "It may also help attain the full diagnostic potential of these scanners, and aid in the transition between new scanners and the old ones."
Session moderator Martine Remy-Jardin, MD, from the University of Lille in France, commented that in clinical practice there are, unfortunately, no clean dividing lines between the indications for CT used in this study such as triple-rule-out or coronary CTA. As for optimizing the protocol using the software, "there is still room for improvement," she said.
For patients with symptoms but no precise clinical suspicions, the TRO is the most comprehensive exam and often the best chance at determining what is going on with the patient, Barraza said.
By Eric Barnes
AuntMinnie.com staff writer
November 29, 2010
Related Reading
Aortic findings at chest CT predict heart disease, events, October 22, 2010
PE risk factor assessment reduces need for CT angiograms, June 16, 2010
Consider screening DVT patients for silent pulmonary embolism: review, May 14, 2010
Is imaging underutilized for diagnosing PE? March 31, 2010
DVT, pulmonary embolism common with superficial thrombosis, February 17, 2010
Copyright © 2010 AuntMinnie.com