One of the largest studies yet comparing medical resource use and outcomes among chest pain patients found that coronary CT angiography (CCTA) reduced medical resource utilization compared to standard care, generating fewer hospital admissions and shorter emergency room stays, researchers reported in the Journal of the American College of Cardiology.
The retrospective study compared matched cohorts of nearly 1,000 patients presenting with chest pain before and after implementation of routine CCTA evaluation. The study team from Stony Brook, NY, and two other institutions found that patients receiving the standard workup for chest pain -- which is to say, mostly observation -- were admitted to the hospital almost five times as frequently as patients receiving CT. The standard workup patients also had significantly longer stays when admitted.
The rates of invasive angiography without revascularization and recidivism were also much higher for patients receiving standard care (JACC, May 14, 2013).
"I think the take-home message is that CT done correctly by experts with the resources to do it correctly on a routine basis is not only safe and feasible, but reduces healthcare resource utilization," said lead author Dr. Michael Poon, from Stony Brook Medical Center, in an interview with AuntMinnie.com.
More than $10 billion in costs
Caring for chest pain is an expensive proposition in the U.S., costing upward of $10 billion a year for some 6 million emergency department (ED) visits. To reduce the problem of overcrowded emergency rooms, some hospitals have implemented chest pain evaluation units, but the care isn't comprehensive or necessarily all that helpful, Poon said.
"It has been a problem and a major dilemma for emergency rooms because for most patients, it's a false alarm," he said. "I would say nine out of 10 are false alarms, but how to pick out that one is very tricky and costly. So what most hospitals tend to do is a one-size-fits-all policy where everybody gets blood tests and an electrocardiogram, and they keep patients in the ED for an extended period of time. So if you come in Friday, you may stay until Monday."
Coronary CTA has been shown to be safe and cost-effective for acute chest pain evaluation in several smaller studies and in three smaller multicenter trials, but those studies have been limited by a lack of CT availability outside of weekdays and office hours, while EDs must operate 24/7, Poon said.
"All of those studies were done in a randomized, controlled fashion and in an artificial environment," where each patient was randomized to either a stress test or CT during weekday office hours, Poon said. "But in real life, there is no such thing; it cannot be done."
More often, chest pain patients get a couple of tests and several hours of observation before they are sent home.
Poon and colleagues from Stony Brook, William Beaumont Hospital, and the University of Toronto wanted to do a "real-world" observational study to show that CT remained cost-effective and efficient for triaging chest pain patients.
The study sought to compare the overall impact of CT on clinical outcomes and efficacy, when comparing CCTA and the hospital's standard evaluation for the triage of chest pain patients, with CCTA available 12 hours a day, seven days a week.
From a total of 9,308 patients with a chest pain diagnosis upon admission, the study used a matched sample of 894 patients without a history of coronary artery disease and without positive troponin or ischemic changes on an electrocardiogram.
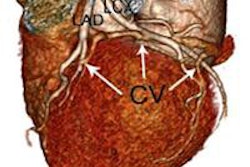
Patients undergoing CT were scanned on a 64-detector-row scanner (LightSpeed VCT, GE Healthcare) following administration of iodinated contrast and metoprolol as a beta-blocker for those with heart rates faster than 65 beats per minute (bpm).
Those with a body mass index (BMI) less than 30 were scanned at 100 kV, while those with a BMI between 30 and 50 were scanned at 120 kV. Retrospective gating was reserved for patients whose heart rates remained above 65 bpm. Obstructive stenosis was defined as 50% or greater lumen narrowing.
CT choice faster, more efficient
The results showed a lower overall admission rate of 14% for CCTA, compared with 40% for the standard of care (p < 0.001). In fact, patients undergoing standard evaluation were 5.5 times more likely to be admitted (p < 0.001) than CCTA patients.
The length of stay in the ED was 1.6 times longer for standard care (p < 0.001) than for CCTA. For patients undergoing CCTA, the median radiation dose was 5.88 mSv.
"We also showed that the recidivism rate is higher for standard of care, meaning that they come back within one month with recurrent chest pain," Poon said. The odds of returning to the ED within 30 days were five times greater for patients in the standard evaluation group (odds ratio, 5.06; p = 0.022).
"In the era of Obamacare, this is a penalty to the hospital; you don't want the patient returning within one month with the same diagnosis," he said. When that happens, "you're not only not getting paid, you have to pay a penalty. It's a double whammy. We also show that downstream invasive coronary angiography is significantly less in the CCTA arm."
More invasive angiography
Patients receiving standard care were seven times more likely to undergo invasive coronary angiography without revascularization (odds ratio, 7.17; p ≤ 0.001), while neither patient group was significantly more likely to undergo revascularization.
"Many physicians use [catheterization] as a way of getting patients in and out of the hospital," Poon said. However, the cost is more than $10,000 per procedure.
The high rate of angiography without revascularization in the standard care group was not seen in the Rule Out Myocardial Infarction/Ischemia Using Computer Assisted Tomography (ROMICAT) I and II trials, where all patients in the standard care group underwent stress testing before angiography was considered, he said.
Poon credited the ROMICAT trials' routine use of stress tests with diminishing CT's relative advantage in resource use. "In the real world, that is not available," he said. The present study, in which only about 20% of the standard care patients underwent stress tests, is more realistic.
Finally, Poon and colleagues showed no difference in rates of myocardial infarction between CT and the standard of care within the first 30 days of follow up. However, that is changing as patients are followed for longer time periods, he noted.
"We see a trend starting to diverge in our next report, which follows [patients] for six months," he said. "You see a lot more acute myocardial infarction in the standard care arm, and we're going to extend it for a year."
The authors concluded that using CCTA to rule out acute coronary syndromes in low-risk chest pain patients is likely to improve doctors' ability to triage patients with the common presentation of chest pain. The result of this approach appears to be fewer hospital admissions, shorter stays, less recidivism, less invasive angiography, and better patient outcomes.
In any case, Poon said, the study method is permanent at Stony Brook University, where the standard of care now incorporates CCTA.
"We didn't stop doing it after the study," he said. "If you look at some of the randomized, controlled studies, they actually went back to the standard of care." They had to because those kinds of protocols are only practical with a grant.