Vasodilator stress cardiac MR (CMR) and 320-detector-row coronary CT angiography (CCTA) both accurately detect obstructive coronary artery disease, and the two tests are also highly concordant, according to the results of a new study in the International Journal of Cardiovascular Imaging.
In 150 patients followed for a year and a half, researchers found a high degree of concordance -- 92% -- between vasodilator stress and CCTA results. Both tests yielded sensitivities and specificities in the 90% percentile for the detection of obstructive disease. Survival rates in patients with negative results exceeded 95% in both tests, reported Dr. Marcus Chen and colleagues from the National Heart, Lung, and Blood Institute (Int J Cardiovasc Imaging, October 12, 2013).
"In a predominantly intermediate-risk group of patients, stress CMR and CTA findings have excellent agreement, and both tests are accurate for the assessment of obstructive [coronary artery disease (CAD)]," Chen said in an interview with AuntMinnie.com. In a study that represents the first direct comparison of the two tests, both were also shown to be highly prognostic, added Chen, who is director of cardiovascular CT at the institute.
Huge problem, limited tests
Suspected obstructive CAD is a huge problem in the U.S., with more than 9 million stress tests and 1 million invasive angiograms performed each year, costing billions of dollars. But stress testing is considered to have limited value for detecting obstructive coronary disease, which has led to greater use of two emerging tests, CCTA and vasodilatory stress cardiac MRI, to evaluate obstructive disease.
The tests are fundamentally different in that vasodilator stress CMR detects ischemia whereas CCTA detects atherosclerosis.
"We're really measuring two different ways of looking for coronary disease," Chen said. "One test [CCTA] measures obstructive disease, and the other measures the consequences of that obstruction. That's the MRI, which is looking to see if the heart tissue itself is getting enough blood flow. Both tests work very well for detecting coronary disease, and the interesting part is that these two high-end tests agree with each other."
The study sought to evaluate the concordance and relative diagnostic accuracy of these two very different tests in 151 patients (average age, 56 ± years). The patients did not have known disease and were referred for noninvasive evaluation of potential obstructive coronary artery disease.
Recognizing that most of the cohort would be unlikely to undergo invasive angiography, the study team assessed the accuracy of CT and MRI by using a combination of subsequent diagnostic tests, revascularization, and major cardiac events that occurred over the follow-up period.
Findings from invasive angiography were then combined with patient outcomes to determine diagnostic accuracy. Chen and colleagues hypothesized that both CCTA and CMR are accurate for diagnosing obstructive coronary disease and are predictive of future events.
After administration of beta-blockers and iodinated contrast to achieve a resting heart rate of 60 beats per minute or less, CCTA images were acquired on a 320-detector-row CT scanner (Aquilion One, Toshiba Medical Systems). Tube voltage and current were adjusted to the patient's body size, and images were reconstructed at 0.5-mm slice thickness with a 0.25-mm increment and kernel FC03. The readers used a dedicated workstation (Vitrea fX, Toshiba) and were blinded to all other results. Stenosis of at least 50% in an artery 1.5 mm or larger was considered positive.
Vasodilator stress CMR was performed on a 1.5-tesla scanner (Avanto or Espree, Siemens Healthcare) using a 32-channel surface coil after administration of 0.5 mmol/kg gadopentetate dimeglumine and dipyridamole 0.56 mg/kg as a vasodilator. Imaging parameters included a saturation preparation pulse, 50º flip angle, 2.3/1.1 msec TR/TE, 128 x 80 acquisition matrix, and 360 x 270-mm field-of-view.
This was followed by the acquisition of cine images and baseline "rest" first-pass perfusion images after more contrast administration, with results read on a Leonardo workstation (Siemens). As with the CTA images, CMR readers were blinded to the results of other imaging modalities and clinical tests, the authors wrote. Stress-induced perfusion defects of any size were considered abnormal. Catheter-based invasive angiography was performed in patients who were positive at either CTA or CMR.
The subjects were followed for an average 450 ± 115 days for cardiovascular events and downstream testing. CTA and CMR agreed in 139 subjects (92%, κ = 0.81, p < 0.001). The 12 discordant cases (a level that did not reach statistical significance) included seven subjects with a positive CCTA and negative CMR result, and five subjects with a negative CCTA and positive CMR.
The prevalence of coronary artery disease was typical of noninvasive test populations: 30% for CTA, 28% at CMR, and 24% at angiography. Compared with invasive angiography, CMR's sensitivity was 93% and CCTA's sensitivity was 98%.
| CCTA and CMR vs. invasive angiography | ||
| Parameter | CMR | CCTA |
| 450-day event-free survival | 97%, nonischemic | 99%, nonobstructive |
| 39%, ischemic | 36%, obstructive | |
| Sensitivity | 93% | 98% |
| Specificity | 96% | 96% |
| Positive predictive value | 91% | 91% |
| Negative predictive value | 97% | 99% |
| Accuracy | 95% | 97% |
"Nonischemic vasodilator stress CMR or nonobstructive coronary CTA were highly concordant and each confer an excellent prognosis," the group reported.
Over the follow-up period, 43 subjects (30%) underwent invasive angiography and 29 major cardiac events occurred: one death, two nonfatal myocardial infarctions, 11 percutaneous interventions, and 15 coronary artery bypass surgeries, the group reported.
Inherent differences
"Myocardial perfusion imaging by CMR or nuclear techniques assesses the physiological significance of CAD, whereas CTA provides anatomic visualization of the location and severity of atherosclerosis," the authors wrote. "The inherent differences in assessing physiology versus anatomy have been used to explain discordant findings between CTA and both SPECT and PET imaging. However, in this study, the correlation between CTA and CMR was excellent (agreement 92%, κ = 0.81) which is consistent with another smaller study."
The results show that CMR has a higher diagnostic accuracy than SPECT. Also, the concordance between CTA and CMR is much higher than that seen with conventional modalities -- for example, echocardiography and SPECT, which yielded 62% concordance with a κ value of 0.25, the group noted.
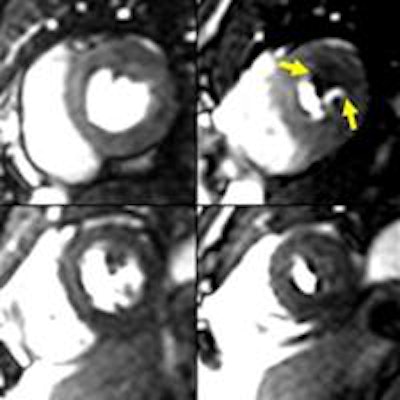
 Images show concordant positive findings on stress CMR (above) and CTA (below) in a 42-year-old man with chest pain. The lateral wall stress-induced perfusion defect on CMR corresponds with the noncalcified severe stenosis involving a large obtuse marginal branch on coronary CTA. These CMR and CTA findings were confirmed on subsequent invasive angiography (bottom) with successful coronary stenting of the severe stenosis. All images courtesy of Dr. Marcus Chen.
Images show concordant positive findings on stress CMR (above) and CTA (below) in a 42-year-old man with chest pain. The lateral wall stress-induced perfusion defect on CMR corresponds with the noncalcified severe stenosis involving a large obtuse marginal branch on coronary CTA. These CMR and CTA findings were confirmed on subsequent invasive angiography (bottom) with successful coronary stenting of the severe stenosis. All images courtesy of Dr. Marcus Chen.


Among the study limitations, the authors noted that the current gold standard, conventional angiography, does not identify lesion characteristics such as length, shape, eccentricity, collateral blood flow, or vasomotor tone, and as a result may misrepresent the physiological significance of lesions, especially intermediate lesions. Also, enrolling subjects who will eventually undergo invasive angiography introduces pretest referral bias because it enriches the cohort with high-prevalence disease subjects, which boosts the number of positive results and potentially exaggerates test sensitivity.
Still, the data are highly applicable to typical heart disease populations, according to the authors.
"The strength of our study is that the predominately intermediate-risk group of patients in this cohort reflects a typical outpatient population, and therefore the prognostic information is broadly applicable," the group wrote.
CMR's advantage is that it offers a comprehensive evaluation of cardiac anatomy. However, CCTA is more widely available and has shorter exam times, though the delivery of ionizing radiation limits the acquisition to a small portion of coronary anatomy. Both tests are accurate for evaluating obstructive CAD, and both confer an excellent prognosis, the group concluded.
"Overall, CT is a little bit more sensitive than MRI, but the advantage of MRI is that it gives you more information than just diagnosing coronary disease," Chen said. "With MRI we can get an assessment of how the heart is contracting, the ejection fraction; you can look at wall-motion abnormalities, you can look at the valves, and with the contrast material, you can look for areas of infarction or scar or fibrosis."
CT has its own advanced assessment tools, but the drive to minimize radiation dose means that most of the time the modality is used to image only a small portion of the cardiac cycle. Even so, there is plenty of future work to do in terms of getting physiologic information from CT and seeing if it compares with MRI, Chen said.