CT radiation dose alerts have their strengths and certainly their weaknesses, according to a study from Boston. But for better or worse, the alerts are mandatory under the Smart Dose (XR-29) rules that took effect last month. So radiologists must comply -- while still looking for ways to improve the new standard.
The study looked at the utility of dose alerts for preventing tissue damage, and it showed that they are broadly useful and do prevent harm to patients, said radiologist Dr. Aaron Sodickson, PhD. But the alerts also suffer from Mack-truck-sized blind spots owing to their one-size-fits-all design that cannot help patients who aren't average-sized.
Dose alerts "offer no mechanism to account for patient size," noted Sodickson, who is section head of emergency radiology at Brigham and Women's Hospital. "So for obese patients, the use of values that exceed the notification levels is likely to occur but may be completely appropriate."
At the same time, smaller patients may be overexposed. Despite these limitations, the standard can certainly be improved over time, Sodickson said in June in a talk at the International Symposium on Multidetector-Row CT (MDCT 2015) in San Francisco.
Comply or pay
There are incentives to comply with the directive. As with other CT scanner features (such as preloaded protocols and DICOM reporting) mandated by Congress as part of the Protecting Access to Medicare Act of 2014, physicians who use older scanners that lack dose alerts will face a 5% reimbursement penalty beginning in 2016 and a 15% penalty beginning in 2017.
 Dr. Aaron Sodickson, PhD, from Brigham and Women's Hospital.
Dr. Aaron Sodickson, PhD, from Brigham and Women's Hospital.Unfortunately, the standard that governs how dose information will be collected and reported is far from perfect, Sodickson said. But it succeeds in its very basic function.
"The intent of these alerts is to present a time-out opportunity for the user to confirm the scan settings" and, thus, prevent tissue damage from overexposure, he said.
Soon after the standard was introduced, the American Association of Physicists in Medicine (AAPM) pitched in to help doctors comply by producing a list of notification-triggering dose values that were intentionally set higher than the American College of Radiology's (ACR) diagnostic reference levels.
For example, AAPM set CT dose index volume (CTDIvol) notification values at 80 mGy for an adult head exam, 50 mGy for a pediatric head study, and 50 mGy for an adult torso study. These rather generous alert levels were designed to provide some leeway in scan doses and hopefully avert serious damage to the patient.
There are actually two kinds of alerts, Sodickson said. There is a dose notification, where a technologist is warned at the time of the scan that a configured threshold might be exceeded for any part of the prescribed scan. Then there is a dose alert, which sounds a warning if cumulative CTDIvol or dose-length product (DLP) values would exceed a certain dose threshold during the scan.
Testing the triggers
How well do they work? Significant shortcomings were revealed in a 2013 study by Sodickson and colleagues that showed a large number of outliers -- that is, patients who received higher-than-expected CTDIvol levels relative to the tube current modulation of similarly-sized patients.
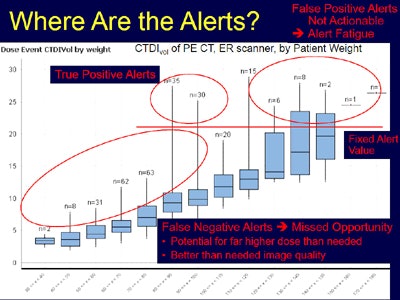
Setting an alert level at a fixed CTDIvol value showed that the most common outliers were false-positive alerts for doses that were completely appropriate for the larger patients who received them.
"These are not actionable alerts, and they lead to alert fatigue," Sodickson said. "If every time we have an alert the technologist needs to ignore it, then they stop paying attention."
At the same time, there were many false negatives, or cases where smaller-than-normal patients received doses higher than they needed, but since the alert level was too high for them, there was no alarm.
 Chart from 2013 study plots CT scans from the emergency department, separating patients by increasing weight into columns from left to right. The results show that necessary alerts for smaller patients receiving relatively high doses (patients within red circle at left) would not have been generated. At the same time, too many alerts would be generated for larger patients (within red circle at right) who exceeded ACR diagnostic reference levels. The small red circle at center represents average-sized patients whose dose alarms would be appropriate. Image courtesy of Dr. Aaron Sodickson, PhD.
Chart from 2013 study plots CT scans from the emergency department, separating patients by increasing weight into columns from left to right. The results show that necessary alerts for smaller patients receiving relatively high doses (patients within red circle at left) would not have been generated. At the same time, too many alerts would be generated for larger patients (within red circle at right) who exceeded ACR diagnostic reference levels. The small red circle at center represents average-sized patients whose dose alarms would be appropriate. Image courtesy of Dr. Aaron Sodickson, PhD.Useful to a point
Dose alerts "remain helpful for high-level screening of institutional techniques to make sure that we're avoiding tissue-damaging effects, and, in fairness, this was the purpose that these were designed for: to reduce tissue-damage effects," Sodickson said.
But in practice, CT technique and therefore patient dose depends very much on patient size.
"So if we want to do meaningful protocol surveillance and optimization, we have to address the size dependence, and outlier detection -- particularly in the torso -- is severely limited if we don't consider patient size," he said.
The results showed an eightfold difference in dose at 120 kV, owing simply to the size of the larger patients, who were appropriately scanned because they need more x-rays to penetrate their bodies, Sodickson said.
A better approach
Going forward, how can the system be improved? The optimal approach to reference levels might be having a scanner that displays a size-specific dose notification value to help confirm that the technique is appropriate, according to Sodickson.
Ideally the data would be available to technologists during training, to radiologists during interpretation and technique review, and to medical physicists during protocol review.
"The ideal metric that I like is the water-equivalent diameter," Sodickson said. "This incorporates patient-specific x-ray attenuation, it is insensitive to body contour variability, and it mirrors the underlying tube current modulation calculations having the tightest distributions in general of CTDIvol and size."