CHICAGO - A new fetal dose-measurement technique ties CT dose index volume (CTDIvol) scanner readouts to size-specific dose estimates (SSDEs), opening a door to greater accuracy in fetal dose measurement, according to a presentation at the 2015 RSNA meeting.
Fetal dose must be estimated when a pregnant woman needs a CT scan, but current dose-estimation techniques are limited to fixed tube current scans, while in practice most exams are conducted with tube current modulation.
In a study of 18 women who were scanned with CT while pregnant, investigators from the University of California, Los Angeles (UCLA) created CTDIvol-to-fetal-dose conversion coefficients for tube-current-modulated CT scans. They found the comparison between water-equivalent-diameter patient sizes and CTDIvol-to-fetal-dose measurements to be both accurate and reliable.
This result tells us that "CTDIvol can properly account for scan technique variation, and a water-equivalent-diameter patient size metric properly accounts for patient size variation," said Kyle McMillan, a graduate student researcher at UCLA, in his talk.
Doctors do their best to avoid them, but "CT scans are sometimes required in pregnant patients -- typically in the case of trauma, such as car accidents," McMillan said. "We need accurate estimates of the dose to the fetus in order to determine if the diagnostic benefit outweighs the risk, however small that risk may be."
The best way to get accurate dose measurements is by accounting for fetus size. A seminal 2008 paper by Angel et al in Radiology described fetal dose as a function of maternal perimeter, fetal depth, and gestational age, but it didn't include tube current modulation (TCM), which is used in most CT scans today, he said.
"We want to include TCM in fetal dose estimates," McMillan said.
The current study aimed to use similar methods to develop patient-specific fetal dose estimates that were independent of scan technique in pregnant patients of various gestational ages, McMillan said.
The 18 pregnant women had a gestational age between 12 and 36 weeks and underwent clinically indicated abdominal and pelvic CT exams. McMillan and colleagues created models of maternal and fetal anatomy from CT image data.
Doses were estimated using Monte Carlo simulation of tube-current-modulated scans of the abdomen and pelvis on 16- and 64-detector-row scanners (GE Healthcare). For each patient, the study team manually segmented topogram images of the uterus (modeled as soft tissue), gestational sac (modeled as water), and fetus (modeled as soft tissue or bone depending on attenuation).
The water-equivalent-diameter method measured attenuation at the image containing the 3D centroid of the fetus, McMillan said. For the Monte Carlo simulations, they used an equivalent-source method to generate scanner-specific filtration and spectrum descriptions, i.e., a simulation based on the specifications of a Somatom Sensation 64 CT scanner (Siemens Healthcare) at 120 kVp and 200 mAs with a standard bow-tie filter.
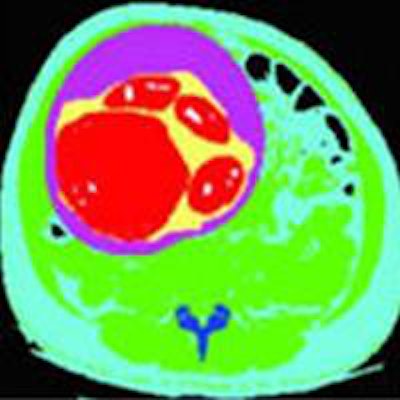
 The CTDIvol-to-SSDE dose conversion technique used voxelized models created from patient images, based on Hounsfield Unit-to-density lookup tables, with the fetus modeled as water, soft tissue, or bone depending on attenuation. Images courtesy of Kyle McMillan.
The CTDIvol-to-SSDE dose conversion technique used voxelized models created from patient images, based on Hounsfield Unit-to-density lookup tables, with the fetus modeled as water, soft tissue, or bone depending on attenuation. Images courtesy of Kyle McMillan.The results showed an exponential relationship between CTDIvol-to-fetal-dose conversion coefficients and patient size. The fetal doses were normalized by scan-specific 32-cm CTDIvol values based on average tube current across the entire scan, i.e., scanner-reported CTDIvol.
This resulted in a technique-independent CTDIvol-to-fetal-dose conversion coefficient for each patient, McMillan said. CTDIvol conversion coefficients were calculated for each of the 18 patients, showing a correlation coefficient of 0.81.
"That's a pretty strong correlation between the fetal dose normalized by the CTDIvol and the water-equivalent diameter determined at the centroid of the fetus," he said.
Admittedly, comparing values from water-equivalent diameter with CTDIvol "is somewhat of a circular validation," McMillan said. But the results show that fetal dose normalized by CTDIvol properly accounts for scan technique variation, and the water-equivalent-diameter patient metric properly accounts for patient size variation.
The question is, "Are these results applicable to other scanners, to other tube current modulation schemes," or only to Siemens scanners? he said. "We will need more definitive proof to answer that."

















