Reporting coronary artery calcium (CAC) on routine chest CT could help clinicians more accurately predict a patient's cardiovascular disease risk and avoid unnecessary additional gated calcium score CT exams, according to a study published in the January-February issue of Current Problems in Diagnostic Radiology.
The results suggest a way cardiovascular care could be improved by identifying patients who could use preventive treatment earlier, wrote a team led by Dr. Joan Chi of the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Manhasset, NY.
"Knowledge of CAC on a prior chest CT may eliminate the need for a subsequent dedicated gated calcium score CT, leading to earlier diagnosis and management of cardiovascular disease as well as decreasing radiation exposure and health costs," the group noted.
Risk assessment
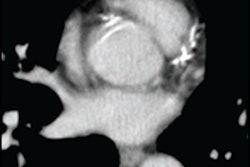
Cardiovascular disease risk assessment can be performed by quantifying CAC using gated CT. Image analysis software produces an Agatston score that helps clinicians predict major adverse coronary events such as a heart attack. But techniques for evaluating CAC on routine chest CT -- like visual estimation and ordinal scoring -- can also predict Agatston score, the group noted (Current Problems in Diagnostic Radiology, January-February 2021, Vol. 50:1, pp. 54-58).
"Current guidelines recommend that CAC noted on nongated chest CTs should be reported," the team wrote. "However, despite these recommendations, CAC is frequently underreported on routine chest CTs."
So could better tracking of CAC on nongated chest CT accurately predict patients' cardiovascular disease burden and help them avoid additional CT imaging? Chi's group investigated the question in a study that assessed 441 patients who underwent gated CT between October 2014 and October 2016.
Of the 441 gated calcium score CT patients, 42 (9.5%) had a prior chest CT. Chi and colleagues compared the presence or absence of coronary calcium and ordinal score on these nongated chest CTs with Agatston scores on gated calcium score CT scans.
Chi and colleagues found the following:
- Of the 42 patients with a gated CT study and a prior ungated chest CT, 29 (69%) had calcium on the ungated exam.
- There was 100% sensitivity and specificity for presence or absence of CAC on prior chest CT and ensuing gated calcium score CT.
- There was an 86% correlation between ordinal scoring on initial chest CT and Agatston score on calcium score CT.
"CAC score quantification is an independent predictor of coronary heart disease, with a higher absolute value correlating with an increased risk of major adverse cardiac events," the researchers wrote. "However, the mere presence of coronary calcium is often a key component in the decision-making process regarding primary preventative therapy, including initiation of lipid-lowering agents. [Our] study shows that many of the subjects with a dedicated gated calcium score study had a prior chest CT which can be readily used to identify the presence or absence of coronary calcium."
Better reporting
Yet of the 29 prior chest CT scans with CAC, 62% had no comment about this in the radiology report, according to Chi's team. The absence of CAC was also not reported in the prior chest CT scans that did not show CAC.
This finding makes clear that reporting must improve, according to the researchers. Adding a dedicated, mandatory CAC section on standardized chest CT report templates "would improve the reporting rates for CAC and possibly reduce the number of dedicated gated calcium score CTs," the group noted.
"Regardless of the indication for a noncontrast CT, the presence of CAC should be mentioned on all routine chest CTs," Chi and colleagues concluded. "Physicians should also inquire about prior chest CTs before ordering gated calcium score CT, and if calcium is not reported they should review the exam with the radiologist or cardiologist to help make clinical decisions without further unnecessary testing."