Stabilizing wounded soldiers in a timely way and evacuating them to the relative safety of larger hospitals away from the front line where they can be imaged and treated appropriately can make all the difference to their survival, but what happens when communications are patchy at best and hospitals have no idea what life-threatening injuries are coming their way?
This is the daily experience of Dr. Andrii Makarenkov, a radiologist at the Zaporizhia Regional Hospital, Ukraine, which receives between three and 10 frontline casualties on a daily basis, most of whom pass through the imaging department.
"Nearly 80% of the Zaporizhia region is occupied now by Russia. Our city is about 15 km from the front line. That's why we're facing patients with combat injuries everyday -- both military and civilians," Makarenkov told AuntMinnieEurope.com. "We can't prepare for their arrival at the hospital as there are no stable connections with evacuation doctors. Admission to the hospital can happen suddenly, after Russian rocket attacks on civilian targets."
 The reading room at Zaporizhia Regional Hospital. From left to right: Dr. Olexandr Davydov, Dr. Andrii Makarenkov, and technician Anna Pustilnik.
The reading room at Zaporizhia Regional Hospital. From left to right: Dr. Olexandr Davydov, Dr. Andrii Makarenkov, and technician Anna Pustilnik.The usual process is for doctors in admissions and in the emergency department to sort patients and decide where to direct them: to the operating room, intensive care unit, or to CT. In the admissions department there is ultrasound or x-ray for those patients that need it, he continued.
The patient arrives accompanied by an anesthesiologist who is responsible for the patient's vital functions during transit. Makarenkov noted that prior to patient arrival, it would be helpful for radiologists to know the nature of the injury, and the time that has passed from injury to examination.
"If doctors have the possibility to tell us what disorder they suspect in each patient, it would be nice. But often they haven't got the opportunity to have such conversations. Especially when massive admission occurs. Plus, there is a shortage of medical personnel as many doctors have been evacuated to western regions of Ukraine," he said.
"We face all types of combat injuries. If the patient is stable enough and doesn't need urgent surgery, then CT is the modality of choice, and we scan from the top of the head to the sit (or sitting) bones. For the head, extremities, and sometimes the lungs, we often perform noncontrast CT, unless we suspect vascular injuries. For whole-body CT, we use contrast enhancement," Makarenkov said.
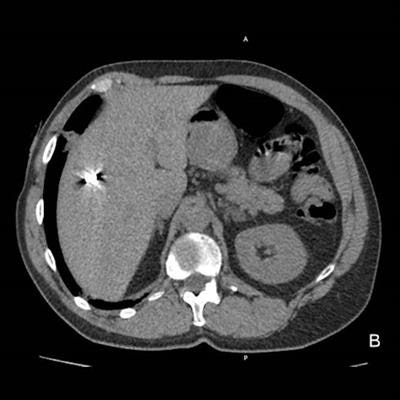
 War injuries like these four cases are encountered on a daily basis at Zaporizhia Regional Hospital. (A) Penetrating gunshot wound. The wound channel passes through the left orbit and the left hemisphere of the brain, containing blood, air bubbles. and metal debris. (B) Shrapnel wound of the liver. (C) Gunshot wound of left hemithorax. The wound channel passes through the left lung with contusion of perifocal parenchyma, left pneumothorax, mediastinal and left subcutaneous and intramuscular emphysema. (D) Gunshot wound of left orbit and left maxillary sinus with multiple metal pellets and hemosinus. Images courtesy of Dr. Andrii Makarenkov.
War injuries like these four cases are encountered on a daily basis at Zaporizhia Regional Hospital. (A) Penetrating gunshot wound. The wound channel passes through the left orbit and the left hemisphere of the brain, containing blood, air bubbles. and metal debris. (B) Shrapnel wound of the liver. (C) Gunshot wound of left hemithorax. The wound channel passes through the left lung with contusion of perifocal parenchyma, left pneumothorax, mediastinal and left subcutaneous and intramuscular emphysema. (D) Gunshot wound of left orbit and left maxillary sinus with multiple metal pellets and hemosinus. Images courtesy of Dr. Andrii Makarenkov.The department's equipment includes a Toshiba Activion16 CT scanner and a stationary angiographic C-arm Toshiba INFX-8000V machine. Medical staff usually continue working during air raids and rocket attack sirens. Sometimes the electricity is cut during CT scans. Contrast media and other consumables are in sufficient quantity for the moment, he noted.
Before the war began, the hospital was an 800-bed regional center, but this capacity has decreased as hospital personnel have been reduced. Makarenkov pays tribute to his radiology team Drs. Olexandr Davydov, Mikola Rudik, Ann Overko, Elena Beregovaya, Evhen Bondarenko, and Helen Mekhtieva, and the technician team: Tetiana Pasechnik, Valeria Moroz, Lidia Latish, Katerina Rybachuk, Alina Kharchenko, Anna Pustilnik, and Karina Zadorozhnia.
Donations from Norway
To help Ukrainian medical and combat teams on the frontline to establish reliable communications, radiologists in Norway have funded a Starlink antenna to establish internet connectivity in one area. The antenna was requested by frontline field surgeon Dr. Yevhenii Nehria, whose wife Dr. Nataliia Nehria, a radiologist, is now living in Berlin.
 Shell injury, treated by field surgeons alerted by internet communication. Image courtesy of Dr. Yevhenii Nehria.
Shell injury, treated by field surgeons alerted by internet communication. Image courtesy of Dr. Yevhenii Nehria.Family friend from Oslo, Dr. Volker Lapczynski, a former vice president of the Norwegian musculoskeletal (MSK) radiological society, launched a GoFundMe page in September 2022, and through the donations from individuals, the project raised over 2,000 euros to cover the purchase of the 480 euro-dish and a year's registration to the Starlink satellite network at 100 euros per month.
Much of the funding was raised through MSK radiologists from the international One Case a Day MSK (ocadmsk.com) mailing list and also participants at the South African Musculoskeletal Imaging Group (SAMSIG) conference in South Africa, Lapczynski noted. The dish was sent to Berlin and then traveled by bus to Nehria's field hospital at the front. Internet coverage via Starlink began on 28 September.
"The antenna provides continuous internet coverage with high speeds of more than 100MB per second," Lapczynski said. "Anyone with the password to the Starlink WIFI can access the internet. Its main purpose is to allow frontline medical teams with no mobile network direct contact with second-line hospitals, to warn them of what type of injuries to expect and prepare for, and also to order supplies from central Ukraine. However, the third prong is that families can stay in touch with loved ones at the front on a regular basis which has revolutionized morale."
Without Starlink, families might not hear anything for months from those volunteering at the front but now, anyone logging in can use messenger services such as WhatsApp and Facebook to message and call. Lapczynski has access to the Starlink app on his phone and says that at any one time there are between five and 20 mobile phones and devices using it to access the web: These might be medics or patients, or simply family members letting relatives know they are still alive.
Access to the internet is proving vital in her husband's field hospital, Nehria told AuntMinnieEurope.com. "My husband and his colleagues treat injured soldiers in the field to stop bleeding, or perform infusions, analgesia, or anti-shock therapy, usually in a medical car or a stretcher on the ground. They then evacuate them to the nearest stabilization center -- any building, medical or other, that has survived the shelling and that is suitable for use -- about 3 km to 15 km from the front."
It's important for his team to communicate with stabilization center doctors via Starlink because they can warn them about the condition of injured soldiers to allow medical colleagues to prepare, she added.
Evacuation planning
Radiologist Dr. Oleksandr Berezovskyi, currently head of the medical service for his military unit at the front and in charge of medical and tactical evacuation of troops, confirmed that due to Russia frequently deploying radio jamming devices, Starlink internet connection was vital.
 This poster, "vanguard of the front" (Передова), was created in recognition of the bravery of frontline medical workers. Courtesy of artist Nikita Titov (https://www.facebook.com/nikitavltitov).
This poster, "vanguard of the front" (Передова), was created in recognition of the bravery of frontline medical workers. Courtesy of artist Nikita Titov (https://www.facebook.com/nikitavltitov).Berezovkyi, who before the war was head of radiology at Odrex medical center in Odesa, explained that internet communication was not just important for emergency doctors to warn stabilization centers of incoming injuries, or the same centers contacting the larger hospitals about arrivals but also for planning patient transport, both for the medical cars getting to military units to treat the injured and ferrying them to the nearest stabilization point, and later for moving stabilized patients to bigger hospitals which can be hours away by road.
"Our evacuation teams need to know about any obstacles on the way to military units or to centers such as destroyed small bridges, in order to plan alternative routes, or so that the troops can mobilize to rebuild a bridge, for example with stones, or remove a road obstacle. I don't how it would be if we didn't have such widely spread Starlink units near the frontline. That's a fact," he told AuntMinnieEurope.com.
Meanwhile, radiologist Dr. Mykola Novikov and his colleagues at the Israeli Oncologic Center (LISOD), 35 km from Kyiv in Pliuty village, Obuhovskiy district, are doing their best to care for cancer patients.
"The Kyiv region seems to be relatively safe for now, but the threat of Russian missiles and drone attacks remains high," he said. "Recent escalation of missile shelling impacted the electrical infrastructure, so multiple healthcare facilities and their respective imaging departments face the risk of blackouts and are currently struggling to establish and improve their solutions for autonomous power sources. I have had no experience of working under fire, but we've experienced missiles and drone hits several kilometers from the hospital and from my residence in Kyiv."
Novikov keeps in touch with fellow radiologists across the country, including ones providing care near or directly at the front lines. He hears that there is a reasonable amount of basic x-ray imaging directly at the front line and in stabilization facilities conducted with analog equipment. However, the demand for digital solutions and PACS for second- and third-line facilities remains high, specifically to store data from different time points and exams for the patients who are being transferred through multiple hospitals for different stages of treatment and/or rehabilitation, he noted.

















