Ultrahigh-spatial-resolution photon-counting detector CT (UHR PCCT) used for coronary CT angiography (CCTA) outperforms conventional energy-integrating detector (EID) CT when it comes to quantifying coronary plaque, researchers have found.
The study showed that UHR PCCT "reduced segmented coronary plaque volume by nearly one-third and improved reproducibility of low-attenuation plaque measurements," wrote a team led by Milán Vecsey-Nagy, MD, PhD, of the Medical University of South Carolina in Charleston. The results were published March 4 in Radiology.
"The importance of quantifying coronary plaque burden has been emphasized previously because plaque burden, not stenosis, is the major predictor of risk of cardiovascular events and death," the group noted.
CCTA is the primary noninvasive imaging technique for the assessment of coronary artery disease, as it allows for the visualization and quantification of plaque, the group noted. The advent of photon-counting detector CT (PCCT) has led to reduced radiation dose and improved spatial resolution; the team referred to previous research that showed that the "improved spatial resolution associated with UHR [PCCT] decreases measured coronary plaque volume, which may improve the previously documented accuracy and reproducibility of CCTA-based plaque quantification."
Vecsey-Nagy and colleagues investigated the efficacy of UHR PCCT for quantifying coronary plaque via a study that included 48 participants with a total of 164 plaques. Patients underwent CCTA with conventional CT imaging, and then also had a UHR PCCT exam within 30 days. The PCCT exam was performed using equivalent or lower CT dose index and equivalent contrast media volume as the conventional CT scan, the group noted. It compared total, calcified, fibrotic, and low-attenuation coronary plaque volumes between the two types of exams and assessed intra- and interreader reproducibility.
The team found the following:
| Performance comparison between EID CT and UHR PCCT for quantifying coronary plaque | |||
|---|---|---|---|
| Measure | EID CT | UHR PCCT | p-value |
| Total plaque volume | 1,084.7 mm3 | 723.5 mm3 | < 0.001 |
| Fibrotic plaque volumes | 627.7 mm3 | 325.4 mm3 | < 0.001 |
| Low-attenuation plaque volumes | 58.1 mm3 | 72.1 mm3 | = 0.004 |
| Calcified plaque volumes | 342.1 mm3 | 344.5 mm3 | = 0.13 |
The group also reported that total, calcified, and fibrotic plaque volumes showed excellent agreement and reproducibility for both UHR PCCT and EID CT, with intraclass correlation coefficients of more than 0.9. Low-attenuation plaque volume had strong intrareader and interreader agreements on UHR PCCT (0.84 and 0.92, respectively) but EID CT showed only moderate and poor intrareader and interreader reproducibility (0.62 and 0.47, respectively).
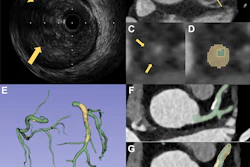
 Representative example shows segmentations performed on the left anterior descending (LAD) artery in a 75-year-old male participant who underwent clinically indicated coronary CT angiography with energy-integrating detector (EID) CT and subsequently underwent photon-counting detector (PCD) CT. Whereas measurements were similar for all plaque components between readers, both investigators noted a substantially lower total plaque volume on the ultrahigh-spatial-resolution scan. The central three-dimensional volumetric image (middle) shows the location of the segmentations. Images and caption courtesy of the RSNA.
Representative example shows segmentations performed on the left anterior descending (LAD) artery in a 75-year-old male participant who underwent clinically indicated coronary CT angiography with energy-integrating detector (EID) CT and subsequently underwent photon-counting detector (PCD) CT. Whereas measurements were similar for all plaque components between readers, both investigators noted a substantially lower total plaque volume on the ultrahigh-spatial-resolution scan. The central three-dimensional volumetric image (middle) shows the location of the segmentations. Images and caption courtesy of the RSNA.
The takeaway? Compared with EID CT, UHR PCCT reduces coronary plaque volume by approximately one-third, with the most pronounced differences in fibrotic components, according to the team, and this quantification of plaque "improves intrareader and interreader reproducibility," it concluded.
The complete study can be found here.