Demonstrating that a coordinated multicenter program can successfully slash CT radiation dose, Michigan doctors cut dose from coronary CT angiography (CTA) studies by more than half statewide, according to the results of a study that will appear June 10 in the Journal of the American Medical Association.
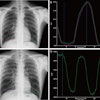
The 15 hospitals participating in the state's Advanced Cardiovascular Imaging Consortium used optimized scanning protocols to achieve a median dose reduction of 53.3% in a wide variety of patients while maintaining image quality, according to the study (JAMA, June 10, 2009, Vol. 301:22, pp. 2340-2348).
The study gives hope to coronary CTA advocates in their effort to counter charges that the radiation dose delivered by CT is too high to make the procedure a routine alternative to conventional coronary angiography for assessing patients who present with symptoms of heart disease. While previous research has also demonstrated that CT dose can be reduced by adjusting scanner protocols, the current study is the first statewide application of a coronary CTA dose-reduction program, demonstrating that the lower coronary CTA doses shown in a handful of single-center studies can be effectively implemented on a large scale.
Coronary CTA's potential
To date, the results of multiple studies suggest that coronary CTA "may definitively exclude the diagnosis of coronary artery disease in a substantial proportion of appropriately selected patients, allowing scarce healthcare resources to be focused on those patients truly requiring long-term medical therapy or expensive invasive procedures," wrote Dr. Gilbert Raff from William Beaumont Hospital in Royal Oak, MI, and colleagues.
However, the authors cited radiation dose as a steep barrier to implementation of coronary CTA on a wider scale. In response, the study aimed to determine whether a radiation dose-reduction program implemented across multiple sites would reduce the radiation dose to patients undergoing coronary CTA over the course of a year, and whether it would affect image quality.
The prospective, controlled, nonrandomized study was performed during a control period (July to August 2007), an intervention period (September 2007 to April 2008), and a follow-up period (May to June 2008) at 15 imaging facilities in Michigan, ranging from small community hospitals to large academic medical centers.
The study enrolled 4,995 sequential patients undergoing coronary CTA for suspected coronary artery disease. Over the course of a year, 4,862 patients (97.3%) had complete radiation data for analysis.
In the control period of the study, the researchers analyzed baseline characteristics of the patients and radiation dose; image quality metrics were then analyzed, and the data were used to develop a set of recommendations for optimized scanning protocols that represent the best practices for low-dose CT scanning. These protocols were distributed to participating centers for use during the interventional phase of the study.
During the study's follow-up phase (the final two months of the study), the measurement data were collected without further intervention and compared with the control period data.
The scanner protocols that were optimized to reduce dose included:
- Scan length minimization
- Uniform beta-blocker preparation
- kVp reduction from 120 to 100 for patients with a body mass index less than 30
- Narrow-window retrospective gating (70 x 70 window) or prospective gating
- Use of tube current modulation
Implementation challenges
The researchers found that implementing the dose-reduction protocols across multiple centers in Michigan was anything but uniform because of the different challenges faced by different centers, they wrote.
"At one site there was a substantial baseline variation from standard coronary CTA practice due to consistent use of higher acquisition voltage (135 kVp); this was quickly corrected," Raff and colleagues explained. "At another site, the problem was more complex; several scanners were involved in the acquisition of cardiac studies at this large institution. Even with an experienced physician and licensed medical physicist providing input, it took time to implement a process involving many technologists performing these examinations at multiple locations."
The primary study outcomes included dose-length product and effective radiation dose from all phases of the scan. Image quality on a four-point scale (1 = excellent to 4 = nondiagnostic) was also examined, as well as the frequency of diagnostic-quality scans.
Dose reductions using optimized protocols
The results showed that "implementation of a best-practice model for scan acquisition was associated with a marked reduction in coronary CTA radiation dose ... and that diagnostic image quality was not impaired," Raff and colleagues wrote.
Compared with measurements acquired during the control period, patients' estimated median radiation dose in the follow-up period was reduced by 53.3% as measured by the dose-length product, which decreased from 1,493 mGy/cm to 697 mGy/cm (p < 0.001). The median effective dose per study was reduced from 21 mSv to 10 mSv (p < 0.001).
The most powerful factors associated with achievement of lower dose was the use of lower tube voltage (from 120 kVp to 100 kVp) and a site study volume of more than 30 cases per month, the authors said. The percentage of cases in which lower kVp was used increased from 13% to 43% (p < 0.001).
Lower heart rates were the third most significant predictor of low radiation dose. Reduction in heart rates through the use of beta-blockers showed a "strong positive association with a decreased radiation dose for each one beat per minute reduction."
Image quality steady despite dose reduction
Despite the reduction in radiation dose, there were no significant changes in image quality during the control period compared with the follow-up period as measured by median image quality ratings. Images acquired during both study phases were reported to have median image quality ratings of 2 (images rated as good).
In addition, the proportion of diagnostic-quality scans showed little difference during both study phases, with 89% (554/620 patients) having diagnostic-quality scans in the control period versus 92% (769/835 patients) during the follow-up period.
Although measured radiation dose was high at the outset of the study, rapid improvement within the first three months "demonstrates how use of existing technology and technical methods is associated with dramatically reduced dosages," Raff and colleagues wrote.
Discussing the study last month at the International Symposium on Multidetector-Row CT in San Francisco, Raff noted that some studies -- mostly single-center -- have achieved dose reductions as high as 80% or more, down to as low as approximately 2 to 4 mSv per exam, with the use of prospective gating and other dose-reduction methods.
But in the present study, he added, most participants were overweight (mean body mass of 29.4), while others had heart rate variations and other limitations that accompany the clinical evaluation of coronary artery disease in consecutive patients at multiple centers. This meant that not all patients could be imaged at 100 kVp or using prospective gating, and for those who could, padding was added to the acquisition window to ensure the ability to perform optimal image reconstruction without having to repeat an exam.
Nevertheless, implementing the program was credited for reducing the scan length -- only 9% of patients had full thorax scans, obtained for either bypass graft imaging and/or triple-rule-out studies, Raff said. The frequency of electrocardiogram modulation rose from 88% to 96% over the course of the study, and the frequency of 100 kVp use rose from 11% to 44% of patients. Finally, there was no change in the percentage of diagnostic scans (95%) following implementation of the program.
"The dose-reduction program involved an educational aspect at every level in the imaging process," the JAMA article concluded. "Without a feedback loop of regular dose measurements and reports, similar monitoring of patient preparation, and appropriate imaging protocols and resultant image quality, there would neither be the opportunity to detect dose elevations nor the ability to improve practice."
By Eric Barnes
AuntMinnie.com staff writer
June 9, 2009
Related Reading
Color-coded CT protocols help reduce pediatric radiation dose, June 4, 2009
Triple-rule-out CT scans benefit from prospective gating, May 28, 2009
SCCT publishes cardiac CTA guidelines, May 7, 2009
Tube current modulation cuts triple rule-out CTA dose, April 15, 2009
320-detector-row CT cuts dose in triple rule-out exams, February 12, 2009
Copyright © 2009 AuntMinnie.com