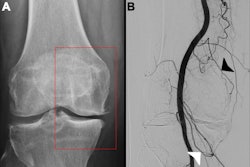
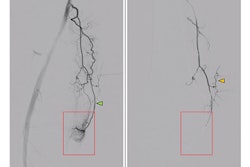
Genicular artery embolization (GAE) is likely a cost-effective treatment for symptomatic knee osteoarthritis compared to radiofrequency ablation or corticosteroid injections, according to an article published September 25 in the American Journal of Roentgenology.
The finding is from a cost-effectiveness analysis using a Markov cohort model that incorporated each treatment’s success and attrition rates, costs, and utility benefit from a U.S. Medicare payer's perspective over four years, noted lead author Daniel Kwak, MD, PhD, of the University of Chicago, and colleagues.
“In all tested scenarios, GAE was consistently the most likely cost-effective treatment option, compared with both RFA [radiofrequency ablation] and CS [corticosteroid injection] over a four-year treatment period,” the group wrote.
Osteoarthritis is a leading cause of chronic pain and long-term disability in adults, with more than 80% of cases involving the knee, and the estimated healthcare costs associated with the disease in the U.S. exceed $80 billion, the authors explained.
GAE and RFA are emerging minimally invasive procedures to treat the disease that may bridge the gap in treatment for patients who are refractory to medical management but are not yet eligible for or decline surgery, they added. Yet while the procedures both have promising supporting data, their wider adoption requires an understanding of their healthcare value relative to costs, the authors noted.
To that end, the authors developed a Markov model based on a de novo network meta-analysis of randomized controlled trials. Utility benefit values were derived at short-term (0.5 to 3 months) and long-term (6 to 12 months) post-treatment follow-ups using an outcome of improved knee pain or function.
In addition, the analyses were conducted at a willingness-to-pay threshold of $100,000 per quality-adjusted life year. The authors performed sensitivity analyses, including when simulating various cost-setting scenarios (office versus hospital outpatient treatment, for instance).
According to the findings, GAE demonstrated higher cost-effectiveness probability compared with RFA: 41.6% to 54.8% versus 18.4% to 29.2%. GAE was also more cost-effective than RFA when clinical success exceeded 51% and the utility value exceeded 0.617 following GAE, and when the GAE quarterly attrition rate was less than 17.4%.
Meanwhile, RFA was more cost-effective when pretreatment utility values exceeded 0.713, the authors reported.
“GAE was consistently the most likely cost-effective treatment option compared to RFA and CS, although clinical success rates, attrition rates, and utility values impact its cost-effectiveness,” the group wrote.
Ultimately, however, interpreting the study’s results in the context of real-world practice is limited, it noted.
“The findings emphasize the significance of clinical success rates, attrition rates, and utility values to the cost-effectiveness of GAE, as well as the need to clarify and optimize these parameters through prudent patient selection and future research initiatives,” the team concluded.
The full article is available here.