NEW ORLEANS - The combination of FDG-PET and ultrasound-guided fine needle aspiration (USFNA) plays a major role in determining how far thyroid cancer has spread to the lymph nodes, according to investigators from Hokkaido University in Sapporo, Japan.
For the post-treatment assessment of thyroid cancer, "whole-body radioiodine 131I scan (RIS) and the monitoring of serum levels of thyroglobulin (Tg) are the methods of choice for postsurgical follow-up," wrote Dr. Kunihiro Nakada and colleagues in a poster presentation at the 2003 Society of Nuclear Medicine conference.
However, when RIS results are negative but Tg levels are still elevated, clinicians still need to localize metastatic tumors in the lymph nodes, they added. While USFNA is an invasive procedure, it does have higher sensitivity and specificity for lymph node metastases from primary head and neck cancer.
Seven men and 31 women (age range, 28-79) were recruited for this retrospective study. They underwent FDG-PET scans on an ECAT EXACT 47/HR+ scanner (CTI/Siemens Medical Systems) after fasting for 6 hours and immediately following an intravenous injection of 185 MBq of FDG. The data was acquired one hour post-injection in a 3-D acquisition mode (emission at two minutes; transmission at three minutes.
"Both attenuation corrected and non-corrected images were reconstructed to be interpreted by three independent nuclear medicine physicians," the authors stated. The readers graded the images on a 5-point scale with 1 for normal, 3 for equivocal, and 5 for abnormal.
The ultrasound exam was performed with either a 7.5 MHz or 10 MHz linear probe. When a lesion exhibited signs of malignancy on the ultrasound and was deemed safe for puncture, USFNA was done using a dedicated, 21-gauge needle.
"Results of FDG-PET and USFNA were correlated with the longest diameter of the lesion (<1 cm = small; 1-2 cm = intermediate; >2 cm = large)," the authors wrote.
For nine patients, final confirmation was done with histologic correlation. Twenty-nine patients were followed-up for at least a year with some type of imaging.
According to the results, a total of 68 metastatic lymph nodes were confirmed, with the majority (38) considered small. There were 15 benign lesions with 6 intermediate sized ones. FDG-PET alone correctly identified 20 small nodes; the addition of USFNA brought that count up to 26. Five out of 15 benign lesions showed positive uptake on FDG-PET. Only one benign lesion was positive on USFNA.
The sensitivity for FDG-PET alone was 80% and 92% for USFNA. When combined, the sensitivity rose to 95%. The specificity was 66% on FDG-PET, 73% on USFNA, and 93% in combination. The accuracy of FDG-PET alone was 78%; the accuracy of USFNA was 92%; together, the accuracy was 95%.
Finally, the positive predictive value of FDG-PET and USFNA was 98%; the negative predictive value was 95%.
"The diagnostic accuracy of FDG-PET is enhanced by the addition of USFNA," the authors concluded. "The combination may be the best tool in the accurate detection of 131I negative metastatic neck nodes from thyroid cancer."
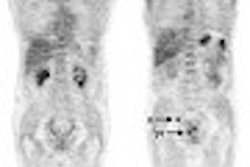
One of the cases involved a 54-year-old male with papillary thyroid cancer. Post-therapy, his 131I scan failed to show an abnormal uptake despite serum Tg levels of 32 ng/ml.
The coronal slice of the FDG-PET scan showed focal uptake in the right paratracheal region. The ultrasound exam showed a corresponding mass lesion where the echo level was bright. The USFNA results were negative. A needle biopsy confirmed that the mass was inflammation and not a tumor.
By Shalmali PalAuntMinnie.com staff writer
June 23, 2003
Related Reading
U.S. PET backers win some, lose some, April 17, 2003
For thyroid applications, iodine-123 looks great, less stunning, October 21, 2002
Copyright © 2003 AuntMinnie.com