
More than 2.2 million people in the U.S. turned up at their doctor's office with complaints of wrist pain in 2005, according to the American Academy of Orthopaedic Surgeons (AAOS). These cases made up 72% of all wrist-related physician visits that year -- and the pain was not related to any specific injury or trauma.
So how many of these wrist issues stemmed from modern-life activities that the human hand is being forced to adapt to, such as typing, mousing, and text messaging?
More than just a handful, based on the anecdotal experience of Dr. Mihra Taljanovic, the head of the musculoskeletal imaging section in the department of radiology at the University of Arizona Health Sciences Center in Tucson. She told AuntMinnnie.com that she has noticed a recent uptick in the number of patients referred to her from private practices for the evaluation of specific wrist and hand-related pathologies.
But sending these patients off for costly MRI and MR arthrography exams, or radiation-laden CT arthrography, is not always feasible. Instead, Taljanovic and colleagues have proposed using ultrasound-based exams as a screening tool for wrist ligaments.
For this prospective study, Taljanovic and colleagues performed sonography of the scapholunate ligament (SLL), the lunotriquetral ligament (LTL), and the triangular fibrocartilage (TFC) disk. The SLL is C-shaped and the LTL is V-shaped, while the TFC disk is part of the part of the TFC complex.
"The two most important intrinsic wrist ligaments are the SLL and LTL. Their disruption may result in pain and substantial instability.... Triangular fibrocartilage disk injury is a common cause of ulnar-sided wrist pain," the group wrote. "Sonography offers the advantage of a dynamic and noninvasive study that is less expensive than MRI and ... MR arthrography. As opposed to ... CT arthrography, sonography offers no radiation to the patient," (Journal of Ultrasound in Medicine, February 2008, Vol. 27:2, pp. 179-191).
Dynamic real-time sonography (Logiq 9, GE Healthcare, Chalfont St. Giles, U.K.) was done on symptomatic wrists in 16 adults. A 9- to 12-MHz linear hockey stick transducer was used because its small size lends itself to scanning the details of wrist ligaments and TFC disk, the authors explained. Ultrasound gel was used in lieu of a standoff pad to accommodate imaging depth. Tissue harmonic imaging also was used.
The SLL was examined with a dorsal approach in a transverse plane (neutral position), as well as with radial and ulnar deviation. The TFC disk was evaluated in a coronal/longitudinal plane with the extensor carpi ulnaris tendon used as an acoustic window. All ultrasound exams were performed by a single musculoskeletal radiologist with 10 years of sonographic experience.
In addition to ultrasound exams, patients also underwent arthrography and MR arthrography of the symptomatic wrist. MR arthrography was done on 1.5-tesla machines (Signa, GE Healthcare) with a 3-inch surface coil. The protocol consisted of T1-weighted imaging with fat suppression in three planes, coronal T1-weighted imaging without fat suppression, coronal proton density-weighted imaging with fat suppression, coronal 3D spoiled gradient-echo imaging with fat suppression, axial T1-weighted imaging without fat suppression, and axial T2-weighted imaging with fat suppression.
Finally, after the MR arthrography study, the sonographic exam of the symptomatic wrist was repeated. The findings of the different techniques were compared. The SLL, LTL, and TFC disk were classified as normal, partially torn/frayed, or torn because "we think that fraying of these structures represents an incidental observation on imaging, which may be of no clinical importance," the authors wrote.
According to the results, for the SLL of symptomatic wrists, the results were concordant for all imaging modalities in 93.75% of the cases. For the LTL, results were concordant for all imaging modalities in 75% of the patients, and for the TFC disk the results were concordant in 81% of the patients.
With MR arthrography used as the reference standard, sonography (US) and sonoarthrography (SA) turned in the following results for sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy.
|
|||||||||||||||||||||||||||||||||||||||||||||||||
Sonography was best at visualizing the dorsal band of the SLL, the authors concluded. In cases of radial-sided wrist pain and a clinically suspected SLL tear, ultrasound can lead to a diagnosis, they stated. While ultrasound's sensitivity for the dorsal band of the LTL only came in at 50%, using sonoarthrography boosted the modality's sensitivity to 83%.
 |
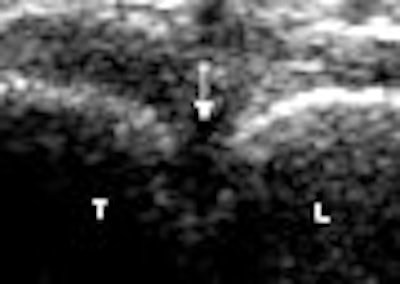
| Torn LTL. Above, transverse sonogram shows the dorsal aspects of the triquetrum (T) and lunate (L). The LTL fibers are not seen (arrow), which is consistent with a tear. Below, the LTL is not visualized on sonoarthrography (arrow) in the same patient. Note hypoechoic fluid extending between the triquetrum and lunate through the LTL tear. Intra-articular contrast improved visualization of the LTL tear. |
 |
| Taljanovic MS, Sheppard JE, Jones MD, Switlick DN, Hunter TB, Rogers LF, "Sonography and Sonoarthrography of the Scapholunate and Lunotriquetral Ligaments and Triangular Fibrocartilage Disk: Initial Experience and Correlation With Arthrography and MR Arthrography" (J Ultrasound Med 2008:12:179-191). Images and caption courtesy of the American Institute of Ultrasound in Medicine. |
Taljanovic said her group has now incorporated sonography of the wrist ligaments into its regular clinical practice. But can sonographic information change the clinical management protocol for these patients -- that is, whether they should be treated surgically or nonsurgically? Taljanovic offered recent examples of how sonography helped guide the patient to the correct treatment.
"I performed ultrasound examinations on two patients with suspected TFC tear (one of them had also clinically suspected scapholunate ligament tear). One of these two patients is allergic to MRI contrast. In this patient, I diagnosed the TFC tear and the patient will probably undergo surgery. I suggested a noncontrast MRI study at 3 tesla for confirmation/correlation if clinically desired," she said.
In another instance, the "patient had sonographic evidence of the TFC disk and scapholunate ligament tear in the symptomatic wrist. However, this patient also had sonographic evidence of significant synovitis in the same wrist, as well as in the extensor compartment tendon sheaths which was more pronounced in the fourth to sixth extensor compartments," Taljanovic added. "This patient also had sonographic evidence of the TFC tear in the contralateral asymptomatic wrist. She will probably be treated for synovitis conservatively and surgery will be contemplated only if these measures fail."
Given that sonography is an operator-dependent exam, Taljanovic told AuntMinnie.com that, on the whole, the exam is reproducible.
"Sonographic evaluation of the dorsal bands of scapholunate and lunotriquetral ligaments is relatively simple and should not be difficult to learn. I believe that a general radiologist should be able to perform it as a screening exam after short training," she said. "However, the evaluation of the triangular fibrocartilage disk and complex is more difficult to perform, and I believe it would require more time and motivation for a general radiologist to learn it."
By Shalmali Pal
AuntMinnie.com staff writer
February 5, 2008
Related Reading
Comprehensive musculoskeletal US exam offers most value, January 3, 2008
Heavy keyboard use won't trigger carpal tunnel woe, November 28, 2007
Making the most of MRI to assess the rotator cuff pre- and postinjury, November 9, 2007
Copyright © 2008 AuntMinnie.com

















