A new study led by Dr. Stamatia Destounis found that women older than 60 years saw changes to their initial cancer treatment plan approximately 50% of the time after undergoing MRI to determine the extent of disease.
Destounis, with a team from Elizabeth Wende Breast Care in Rochester, NY, found that MRI detected additional cancer in 42% of subjects, found atypical and potentially high-risk results in 11%, and had a positive lymph node rate of 23%.
She presented the results at the recent American Roentgen Ray Society (ARRS) annual meeting in Washington, DC.
Benefits of breast MRI
Previous research has found that MRI can detect additional ipsilateral and contralateral lesions in patients recently diagnosed with breast cancer, and it can assist in surgical planning, Destounis noted in her talk. MRI has also been shown to have higher sensitivity than mammography and ultrasound.
The current study was modeled after research published earlier this year on presurgical breast MRI's effects on surgical planning. The prior research found that MRI changed the surgical plan in 24% of women (mean age, 59.4 years) due to the modality's additional findings (Breast Journal, March/April 2013, Vol. 19:2, pp. 134-141).
In that study, led by Dr. X. Cynthia Fan, PhD, from Windsong Radiology Group in Williamsville, NY, 266 lesions in 171 patients were recommended for biopsy. In all, 238 biopsies were performed on 151 patients.
MRI detected 84 additional cancerous lesions in 66 patients and 47 additional high-risk lesions in 39 patients. There were 60 cancerous lesions in the ipsilateral breast, and 24 cancers found in the contralateral breast.
While MRI has proved useful in surgical planning, Destounis added that "studies to date have not reviewed extensively women 60 years of age and older."
"We chose to review our patient outcomes to demonstrate the importance of performing extent-of-disease MRI in women 60 and older," she said.
Retrospective review
The retrospective study by Destounis and colleagues reviewed patients 60 and older who had an MRI between December 2003 and December 2011 to determine extent of disease.
Of the group, 310 patients had a new lesion found on MRI; 243 of these patients met the inclusion criteria for the study, representing a total of 271 MRI findings.
The researchers collected data including lesion size on mammography, ultrasound, and MRI, as well as any additional findings on MRI. Targeted ultrasound findings, core biopsy and pathology, type of surgery, and lymph node status also were noted.
All 271 findings were biopsied: 127 were with MRI (47%), 103 were with ultrasound (38%), 21 (8%) were stereotactic biopsies, and 20 (7%) involved fine-needle aspiration cytology.
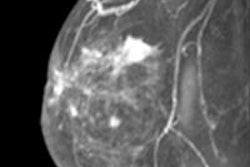
 Known subareolar invasive ductal carcinoma as seen on sagittal MRI. All images courtesy of Dr. Stamatia Destounis.
Known subareolar invasive ductal carcinoma as seen on sagittal MRI. All images courtesy of Dr. Stamatia Destounis.Destounis and colleagues identified 115 malignant cancers (42%) in the retrospective review. Of those, 83 lesions were in the ipsilateral breast and 32 were in the contralateral breast. The group also found 127 benign lesions and 29 atypical/high-risk lesions.
Analyzing the 83 ipsilateral malignant lesions further, 46 were in the same quadrant as the original lesion, 29 were in a different quadrant, and eight were metastatic lymph nodes, according to the researchers.
Of the 29 atypical findings, 12 were contralateral to the original cancer and 16 were ipsilateral (nine lesions in the same quadrant and seven lesions in a different quadrant). There was one ipsilateral lymph node.
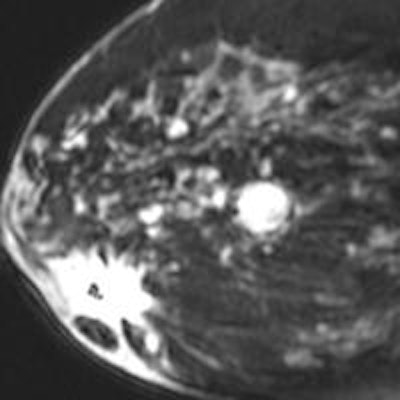
 MRI shows a new lesion found superiorly in the breast. The lesion was subsequently biopsied, revealing another focus of invasive ductal carcinoma.
MRI shows a new lesion found superiorly in the breast. The lesion was subsequently biopsied, revealing another focus of invasive ductal carcinoma.Overall, among the 243 initial patients, 10 women chose not to undergo surgical excision. As for the remaining 233 individuals, MRI changed surgical management in 111 cases (48%), and positive lymph nodes were found among 55 patients (23%).
In conclusion, Destounis said breast MRI's ability to detect the extent of cancer was beneficial in patients older than 60, given that additional cancers were found in 42% of women and atypical results in 11%. The findings led to a change in management in 48% of cases.