It is always a shock when a young, fit athlete dies unexpectedly. Thoughts immediately focus on a cause or unforeseen reason for the sudden loss of a seemingly healthy life, and what could have been done to prevent the tragedy.
Despite technological advances in imaging in recent years, a new review has concluded that cardiac imaging cannot yet be recommended as a first-line screening tool for athletes who show no obvious signs of coronary abnormalities.
The group does, however, suggest that cardiac imaging can be beneficial for athletes with a family history of coronary issues, or who exhibit clinical symptoms and show evidence of abnormalities on an electrocardiogram (ECG).
"While it is imperative that we continue our efforts to safeguard athletes, we must also recognize the current limitations of our tools in predicting [sudden cardiac death (SCD)] in low-risk populations," wrote lead author Dr. André La Gerche, PhD, from St. Vincent's Hospital in Melbourne, Australia, and colleagues from the U.S., Belgium, Finland, and the U.K. (JACC: Cardiovascular Imaging, September 2013, Vol. 6:9, pp. 993-1007).
Sudden cardiac death
Previous research has estimated the incidence of sudden death in athletes younger than 35 to be between 0.6 and 3.6 deaths per 100,000 individuals per year, with the majority of those deaths due to cardiovascular causes (Circulation, April 2011, Vol. 123:15, pp. 1594-1600).
For unknown reasons, the risk of sudden cardiac death is approximately 10 times greater for men than women, and it is also greater among competitive athletes than nonathletes. The chance of sudden cardiac death is also higher among people older than 35 who participate in sports and is highest for those in their 40s (Circulation, August 2011, Vol. 124:6, pp. 672-681).
However, "athletes represent a group in whom the risks of cardiovascular events and SCD are extremely low," La Gerche and colleagues wrote. "The causes of SCD are relatively diverse and are not accurately identified by any one imaging test, especially in the middle-aged athlete who represents a substantial proportion of competitive sports participation."
Past studies in the general population have shown that approximately 0.5% of people with a median age of 51 years who are asymptomatic for heart issues have significant coronary artery disease, the authors noted.
"The predictive value of any imaging modality is likely to be poor given this very low disease prevalence," they wrote. "For example, if the imaging modality were 95% sensitive and specific, the predictive value of the test would only be 9%. In other words, 91% of 'abnormalities' identified on screening could be expected to represent a false positive."
The promise of cardiac MRI
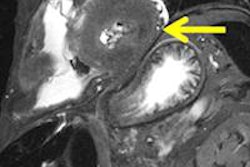
In evaluating different options for screening, La Gerche and colleagues wrote that cardiac MRI has "considerable promise" for asymptomatic athletes. Compared with echocardiography, cardiac MRI can better assess the structure and function of the heart's chambers. It can also provide tissue characterization through T2-weighted imaging of acute swelling or edema, while delayed gadolinium enhancement can evaluate the presence of any fibrosis.
Thus, the authors noted, cardiac MRI should be considered the "most comprehensive imaging modality" to eliminate the presence of coronary disease, making it very valuable for assessing symptomatic athletes.
"However, the relative expense and limited availability of [cardiac MR (CMR)] make it less suitable for broad-based screening and the specificity of CMR testing in athletes with little pretest probability for disease is not sufficiently high to preclude a significant burden of false-positive results," they wrote.
Several recent studies have touted the efficacy of delayed gadolinium enhancement to evaluate the myocardium of seemingly healthy athletes. The studies theorized that small areas of enhancement found in 12% to 50% of well-conditioned athletes could indicate fibrosis due to extreme physical training; however, data remain limited.
La Gerche was the lead author of a 2012 study that used delayed gadolinium enhancement and found that intense endurance training, such as conditioning to run a marathon, can cause acute dysfunction of the heart's right ventricle. Chronic structural changes and reduced right ventricular function were evident in healthy athletes in the study, which recommended further research to validate the results (European Heart Journal, April 2012, Vol. 33:8, pp. 998-1006).
Screening options
Regarding other imaging modalities, La Gerche and colleagues wrote that echocardiography is a "logical candidate" to screen for potential cardiac abnormalities because it is inexpensive and accessible. However, a misdiagnosis could cause financial and psychological side effects for an athlete, they added.
One area in which echocardiography may have benefit is in the diagnosis of hypertrophic cardiomyopathy -- a significant cause of sudden cardiac death in young athletes, according to the authors. But while severe cases of hypertrophic cardiomyopathy could be identified by echocardiography and ECG, these cases are probably rare in highly trained athletes, who would require "more sensitive diagnostic tools" such as cardiac MRI to detect milder concerns, they noted.
La Gerche and colleagues also warned of the financial cost of screening a low-risk population through coronary artery calcium scoring, and the potential for adverse contrast reactions and radiation exposure with CT coronary angiography make this less than ideal as well.
"At present, we have an incomplete understanding of what constitutes the normal range of cardiac morphology and function among athletes of all ages and ethnicities," they concluded. "This is especially true for novel techniques and imaging modalities other than the most basic echocardiographic measures."
They added that atypical findings such as significant cardiac dilation or small areas of delayed gadolinium enhancement may cause unnecessary worry in an asymptomatic athlete who has a very small risk of sudden cardiac death.
"Therefore, we do not believe that cardiac imaging can be recommended as a first-line screening tool," they wrote. "Rather, patient-specific investigations should be focused on evaluating those athletes in whom clinical suspicion is raised by symptoms, family history, clinical exam, and/or abnormalities on ECG."