Cardiac MRI scans showed that 15% of competitive athletes who had recovered from COVID-19 disease had signs of myocarditis on their images, according to a study published September 11 in JAMA Cardiology.
The findings are sobering, wrote a team led by Dr. Saurabh Rajpal of Ohio State University in Columbus. Yet they also highlight that cardiac MRI (CMR) offers an effective way to assess whether athletes can return to competition.
"Cardiac magnetic resonance imaging has the potential to identify a high-risk cohort for adverse outcomes and may, importantly, risk-stratify athletes for safe participation because CMR mapping techniques have a high negative predictive value to rule out myocarditis," the investigators wrote.
Of late, researchers have expressed alarm regarding COVID-19's long-term impact on athletes. In July, a German team found that MRI showed cardiac involvement in 78% of recovered COVID-19 patients and continued myocardial inflammation in 60%.
"Recent studies have raised concerns of myocardial inflammation after recovery from coronavirus disease 2019 ... even in asymptomatic or mildly symptomatic patients," Rajpal and colleagues noted.
So Rajpal's group sought to further investigate if the use of cardiac MRI in competitive athletes who had recovered from COVID-19 could identify myocarditis. Their study included 26 athletes (mean age, 19; 57.7% male) who tested positive for COVID-19 between June and August and underwent cardiac MRI.
Cardiac MRI sequences that were used included cine, T1 and T2 mapping, extracellular volume fraction, and late gadolinium enhancement. Sports represented among study participants included football, soccer, lacrosse, basketball, and track. None of the athletes required hospitalization during their illness, and only 12 were symptomatic.
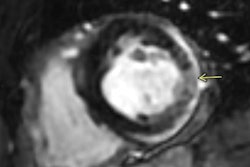
Of the 26 athletes, four (15%) had cardiac MRI findings "consistent with myocarditis," the group found. Two of these had mild COVID-19 symptoms and two were asymptomatic. The researchers also discovered that 30% of study participants had late gadolinium enhancement without T2 elevation, which suggested prior heart muscle injury.
The group acknowledged a few limitations to the study, including lack of baseline CMR imaging and variation in the timing of the exam from positive COVID-19 test results.
"Athletic cardiac adaptation could be responsible for these abnormalities [found on CMR]; however, in this cohort mean ... T2 in those with suspected myocarditis was 59 milliseconds versus 51 milliseconds in those without, favoring pathology," the team wrote.
More study is needed to determine COVID-19's impact on the heart in athletes as the pandemic continues, according to the authors.
"While long-term follow-up and large studies including control populations are required to understand CMR changes in competitive athletes, CMR may provide an excellent risk stratification assessment for myocarditis in athletes who have recovered from COVID-19 to guide safe competitive sports participation," they concluded.