Inflammatory heart disease is rare among professional athletes with prior COVID-19 infection who received systematic return-to-play cardiac screening with imaging and other tests, according to a study published online March 4 in JAMA Cardiology.
The multicenter cross-sectional analysis included return-to-play cardiac testing performed between May and October 2020 on 789 professional athletes who had tested positive for COVID-19. The researchers, led by Dr. David J. Engel of Columbia University Irving Medical Center, found evidence on imaging of inflammatory heart disease that resulted in restriction from play in just five athletes. There was no evidence of adverse cardiac events in the athletes who underwent cardiac screening and resumed play.
"While long-term follow-up is ongoing, few cases of inflammatory heart disease have been detected, and a safe return to professional sports activity has thus far been achieved," the group wrote.
Previous research has found that athletes who recovered from COVID-19 still had signs of chronic conditions such as myocarditis on imaging scans. An Ohio study found that 15% of competitive athletes had myocarditis on cardiac MRI, and a report from Pennsylvania also noted signs of the condition. The findings prompted concern about whether it was safe for athletes to return to play after they had recovered from COVID-19.
In the current study, the authors noted that professional sports leagues in North America (soccer, baseball, hockey, football, and basketball) were among the first to return to full-scale sport activity during the COVID-19 pandemic. In light of the previous research, pro leagues implemented a conservative return-to-play cardiac testing program that followed the American College of Cardiology's May 2020 recommendations for all athletes testing positive for COVID-19.
The testing program included troponin testing, electrocardiography, and resting echocardiography. Those with abnormal screening test results were referred for additional testing that included cardiac MRI and/or stress echocardiography.
In the study, Engel and colleagues identified a total of 460 athletes (58.3%) with prior symptomatic COVID-19 illness, while 329 (41.7%) were asymptomatic or minimally symptomatic. The initial cardiac screening tests raised concern for potential COVID-19-associated cardiac injury in 30 athletes.
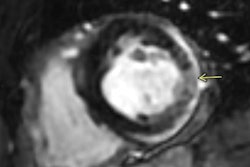
Of these, five athletes (0.6%) ultimately had cardiac MRI findings suggesting inflammatory heart disease (myocarditis in three cases; pericarditis in two cases) that required restriction from play. No adverse cardiac events occurred in athletes who underwent cardiac screening and resumed professional sport participation.
The study results indicate that return-to-play COVID-19 cardiac testing that includes medical imaging can help athletes and sports leagues manage a safe return to competitive sports, according to the authors.
"It is important to note that none of the athletes in this cohort were clinically assessed as having severe COVID-19 viral illness," they wrote.
The authors also noted several study limitations, including the fact that nearly all of the athletes (95%) were men and that some tested positive for COVID-19 early in the pandemic (during the off-season) and did not have to report to training camps until weeks after the initial illness.
However, this reporting of systematic cardiac screening, while not generalizable to all athletic populations, can provide clinical guidance for other athletic organizations who are preparing and optimizing return-to-play protocols.
"Similar studies of other athletes, including pediatric, collegiate, and masters-level athletes, are required," the authors concluded. "Longitudinal assessment of athletes with prior COVID-19 infection remains necessary to enhance our understanding of the short-term and potential long-term pathologic cardiac sequelae of COVID-19 infection."