For patients with stage I uterine cancer, the standard treatment -- hysterectomy with or without lymph node dissection -- is drastic, but the results are quite positive. Numerous studies have shown an excellent survival rate for these women. However, many patients have co-morbidities that preclude them from undergoing surgery. A feasible option for these women is brachytherapy.
In a talk at the 2005 American Brachytherapy Society (ABS) meeting in San Francisco, Dr. Ajay Bhatnagar shared his group's experience with a multichannel uterine applicator for brachytherapy, also known as the Rotte-Y applicator.
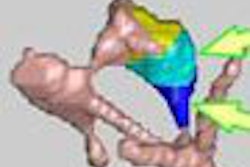
"This two-channel applicator gives reverse pair distribution, allowing for better coverage of the uterus especially in the lateral dimension," said Bhatnagar, who is from the University of Pittsburgh Cancer Institute in Pennsylvania. The applicator "allows superior coverage of the larger uterine size ... and may lead to improved local control."
For the group's study, conducted from 1997 to 2004, 27 patients (median age 70) with stage I inoperable uterine carcinoma received high-dose brachytherapy using the Rotte-Y applicator. Of these 27, 19 patients also received whole pelvic external beam radiation therapy (EBRT) with a median dose of 45 Gy. Patients were selected to receive EBRT based on tumor grade, uterine size, and myometrial invasion determined by MRI, Bhatnagar stated.
"The median uterine width was 6 cm," he said. "Most of our patients did have grade 1 disease; patients with grade 2 and 3 also received external beam."
Patients were given general anesthesia and were immobilized during the procedure. The Rotte-Y applicator was applied under ultrasound guidance. The median length to the applicator was 60 mm, and the angle between the two channels was 45 degrees. Following applicator placement, the patient underwent a CT scan for verification and also to assess uterine width, he said.
For brachytherapy planning, points A, W, and S were calculated using a 14-point software system with optimization mode. Point W was 2 cm below the tip and half the uterine width laterally, with a median number of 34 dwell positions at half-millimeter spacing, he explained. The dose scheme for brachytherapy alone was 7 Gy/bid for a total of 35 Gy. The dose for EBRT was 4 Gy per fraction for a total dose of 20 Gy.
"The median dose for point A was 100% of prescribed dose. The median dose of point W and S were 105% and 89%, respectively," Bhatnagar said. "The median bladder dose was 90% of the prescribed dose and the rectal dose was 46%."
According to the results, the local disease control rate in these patients was 81% based on a median follow-up of 24 months. Three patients with grades 2 and 3 disease developed local recurrence at clinical assessment. "So no patients that had high-dose brachytherapy alone had a local recurrence," he said.
Two patients died within two months of the procedure because of cardiovascular events. Although cardiac complications can be associated with patient immobilization during treatment, these cases were not within the accepted time frame for postprocedural problems, Bhatnagar explained.
Late toxicity occurred in 10% of the cases with one patient (grade 3) with rectal toxicity and one patient (grade 3) with small bowel toxicity.
"The five-year actuary disease specific survival was 73%, and the actual overall survival rate was 45%, which was quite unusual since we usually see these numbers inversed. The reason for seeing a lower overall survival was the fact that these patients died of other co-morbidities," he said.
The research group will continue to follow these women, Bhatnagar said. Patients will be seen every three months for the first year and then every six months thereafter.
ABS session moderator Dr. D. Jeffrey Demanes said that he has used the Rotte-Y applicator in uterine cancer patients, but under conscious sedation on an outpatient basis. In his experience, Demanes said he found the technique to have limited value in patients with larger uteruses. Bhatnagar responded that his group found the exact opposite to be true -- that the applicator was particularly suitable for the larger uterus. However, he pointed out that women with larger uteruses also received EBRT.
By Shalmali Pal
AuntMinnie.com staff writer
July 13, 2005
Related Reading
Urologist promotes brachytherapy for prostate cancer, May 3, 2005
Contrast entry into blood vessel during HSG no cause for alarm, May 5, 2005
Breast and uterine cancer reduced in women with AIDS, April 19, 2005
Copyright © 2005 AuntMinnie.com