The source of the painful snap in snapping hip syndrome can be visualized using dynamic ultrasound, according to South Korean researchers.
Researchers from the Eulji University School of Medicine in Seoul and the Keimyung University School of Medicine in Daegu published a rare radiologic report on the syndrome in the Journal of Ultrasound in Medicine (July 2002, Vol.21:7, pp. 753-758).
Snapping hip syndrome typically occurs in young adults, and often in those who are athletes or dancers. Hip pain and an audible snap are experienced as the patient walks or otherwise moves the hip. This "external" snapping hip is distinct from internal snapping hip caused by snapping of the iliopsoas tendon over the iliopectineal eminence, and intra-articular snapping caused by joint abnormality, the authors note.
The researchers examined five patients with apparent snapping hip syndrome, two of whom were experiencing the syndrome bilaterally. The three male and two female patients ranged in age from 14 to 32. One was a ballet dancer and another was a recreational runner; the others had no history of sports activity. Other than experiencing hip pain from 6 to 18 months, the patients were healthy.
The ultrasound exams were conducted using a phased-array linear 5- to 12-MHz transducer (HDI 3000; Philips Ultrasound, Bothell, WA). After obtaining images of the patients in stasis, the experienced musculoskeletal sonographers used two approaches for the dynamic imaging.
In 5 of 7 cases, dynamic studies were performed during flexion and extension of the hip in the adducted state with the transducer in the transverse plane over the greater trochanter. In the other 2 cases, dynamic imaging was done with the hip in the adducted and internally rotated state and then in the flexed and externally rotated state.
In 4 cases the patients were imaged while standing on the contralateral leg to more effectively reproduce the snap that would occur while standing or running.
"This suggests that weight bearing and contraction of the gluteus maximus muscle are important for generating the external snapping hip," the researchers wrote.
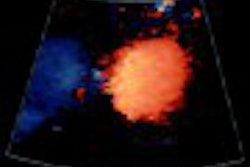
Dynamic sonography revealed the cause of the external snapping hip in each case, the researchers found. In 5 of 7 patients, the cause was shown to be an abnormal jerky movement of the iliotibial band overlying the greater trochanter. In the other 2 cases, the syndrome was caused by a jerky movement of the gluteus maximus muscle during hip motion, the authors wrote.
"The iliotibial band was observed as a hyperechoic (n = 2), hypoechoic (n = 2), or thickened and hypoechoic (n = 1) structure superficial to the greater trochanter," they stated. "No correlation was found between the duration of symptoms and the presence of signs of tendinopathy."
"Abrupt movements of the iliotibial band or the gluteus maximus muscle correlated with the painful click reported by the patients," wrote the authors. "The click could be observed by the examiner through the ultrasonic transducer at the posterior side of the greater trochanter, and was confirmed by the patient when the iliotibial band or gluteus maximus muscle clicked." No iliopsoas tendon or joint abnormality was detected in any of the cases.
Although patients in the study also underwent plain x-rays and some MRI exams, the researchers opined that "once the external snapping hip has been shown in the appropriate clinical setting, no additional imaging study may be required before treatment." External snapping hip syndrome can be treated with rest, moist heat, stretching exercises, and anti-inflammatory drugs. Local anesthetics and steroids may also be injected into the trochanteric bursa. In cases that don’t respond to conservative treatment, surgical procedures can be performed.
By Tracie L. ThompsonAuntMinnie.com contributing writer
August 21, 2002
Related Reading
Multiplanar reformatting may reduce slice views for CT arthrography, March 22, 2002
Ultrasound treatment helps Olympians recover quickly, February 18, 2002
Copyright © 2002 AuntMinnie.com