Thanks to its high negative predictive value, ultrasound elastography with intrinsic compression may be able to reduce by one-third the number of unnecessary biopsies performed on calcified thyroid nodules, according to research published in the October issue of Ultrasound in Medicine and Biology.
In a study involving 65 calcified thyroid nodules, a team of researchers led by Dr. Min-Hee Kim of Catholic University in Korea found that elastography yielded 95.8% negative predictive value in detecting malignancy. Furthermore, more than one-third of biopsies on calcified nodules could have been avoided based on elastography results.
"Intrinsic compression elastography can be used in conjunction with B-mode [ultrasound] to reduce the number of [fine-needle aspiration] biopsies of calcified thyroid nodules," wrote Kim and colleagues, who also came from the University of Washington and Pohang University of Science and Technology.
Confounding calcification
Although calcification in thyroid nodules is an important ultrasound feature that suggests malignancy, and current major guidelines strongly recommend that calcified nodules larger than 5 mm be biopsied, calcification can be present in both malignant and benign nodules. As a result, many benign nodules end up being biopsied unnecessarily (Ultrasound Med Biol, October 2014, Vol. 40:10, pp. 2329-2335).
Ultrasound elastography has been shown in a number of studies to provide high sensitivity and specificity for detecting malignant thyroid nodules. But the lack of interobserver agreement in elastography -- due to variability in data acquisition and scoring -- is a major reason why the method has not been widely adopted in clinical practice, according to the group.
Standard elastography utilizes external compression, with the pressure of the transducer providing the tissue compression that results in the tissue strain measured by elastography. But other researchers have found that elastography utilizing intrinsic compression -- with pressure provided by forces inside the body such as carotid artery pulsation -- could offer better performance. The payoff would be better interobserver and intraobserver agreement.
As a result, the team sought to determine if intrinsic compression elastography could perform well for characterizing thyroid nodules with calcification. The researchers recruited 188 patients with 229 thyroid nodules who were referred to Seoul St. Mary's Hospital from May 2011 through January 2012 for a fine-needle aspiration (FNA) biopsy.
All patients received both ultrasound and elastography exams prior to FNA biopsy. B-mode images were acquired using an iU22 ultrasound system (Philips Healthcare) with a 5- to 12-MHz high-resolution linear probe.
Blinded to the patient's clinical information as well as cytologic and elastography results, a radiologist with 15 years of experience retrospectively reviewed the B-mode ultrasound images and extracted nodule features such as echogenicity, margin, shape, and presence of calcification, according to the researchers. Based on those ultrasound features, the nodules were categorized into three groups: benign, indeterminate, and suspicious for malignancy.
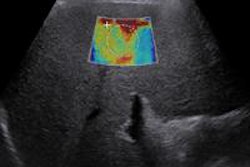
The elastography studies were performed by three endocrinologists with more than one year of experience with intrinsic compression elastography. An Accuvix XG (Samsung Medison) scanner with an L5-13 linear transducer was used in the study, and no external compression was performed while the ultrasound data were acquired, according to the team.
The researchers employed a quantitative scoring method -- elastic contrast index (ECI) -- for the elastography results; a higher ECI value suggests a stiffer nodule and an increasing likelihood of malignancy. A minimum of two ECI measurements were gathered in the imaging plane that showed the thyroid nodule's largest diameter in the transverse view, according to the authors.
Diagnostic accuracy
Next, the researchers determined elastography's diagnostic accuracy by varying the ECI cut-off value in order to find the sensitivity and specificity combination that yielded the maximum geometric mean (sensitivity multiplied by specificity) in detecting malignant nodules. They also calculated positive and negative predictive values.
Of the 196 nodules in the study, 42 were malignant; all were papillary thyroid carcinoma. The mean nodule size was 9 ± 4.17 mm for malignant nodules, significantly smaller than the 11.31 ± 6.1 mm mean size for benign nodules.
The researchers observed that the mean ECI value of malignant nodules (4.51 ± 2.22) was significantly higher than the value for benign nodules (2.98 ± 1.47, p < 0.001). They then calculated elastography's performance, with a mean ECI cut-off value of 3.11 indicating malignancy.
| Elastography performance based on nodule size | ||||
| Sensitivity | Specificity | Positive predictive value | Negative predictive value | |
| All nodules | 81% | 63.6% | 37.8% | 92.5% |
| Nodules < 1 cm | 73.1% | 56.9% | 34.9% | 84.1% |
| Nodules ≥ 1 cm | 93.8% | 68.5% | 34.9% | 98.4% |
The radiologist classified four of the 65 (45 benign and 20 malignant) nodules with calcification as benign; three of the four were found to be benign under elastography. The remaining 61 nodules with calcification were categorized as either indeterminate (29) or suspicious for malignancy (32). With elastography, however, nine of the 32 nodules classified as suspicious for malignancy were determined to be benign, a diagnosis that was confirmed by biopsy.
Furthermore, 12 of the 29 cases that were considered by the radiologist to be indeterminate were judged to be benign on elastography. Biopsy results confirmed the benign diagnosis in 11 of 12 cases; one malignant nodule with rim classification was incorrectly classified as benign using elastography, according to the group.
Elastography's performance in nodules with calcification was as follows:
- Sensitivity: 95%
- Specificity: 51.1%
- Positive predictive value: 46.3%
- Negative predictive value: 95.8%
In all, 23 benign calcified nodules (51.1% of benign calcified nodules) were correctly classified by elastography, whereas only four (8.9%) were correctly classified by B-mode ultrasound, the authors wrote.
The study demonstrates a potential role for elastography in the management of calcified thyroid nodules, according to the researchers.
"With the use of elastography on those calcified nodules, for which B-mode [ultrasound] has low specificity (i.e., 8.9%) in detecting malignancy, FNA biopsy could have been avoided in 23 (35.4%) of 65 calcified nodules," they wrote. "In terms of reducing the number of FNA biopsies, our study found that elastography had a clinical impact similar to that reported in a previous study that evaluated the usefulness of elastography in calcified breast lesions."