
Real-time shear-wave elastography (SWE) isn't just effective for assessing fibrosis in patients with hepatitis C. It also performs well in a broader patient population with diffuse liver disease, according to research published in the September issue of the American Journal of Roentgenology.
In a prospective study of 50 unselected patients with diffuse liver disease, a research team led by Dr. Michael Beland of Rhode Island Hospital found that real-time SWE could accurately predict significant fibrosis (stage ≥ 2) in patients with and without hepatitis C.
"There appears to be value in using SWE in all patients with diffuse liver disease from etiologies other than viral hepatitis," Beland told AuntMinnie.com.
Adding another level
Tissue elasticity imaging has the potential to add another level to ultrasound interpretations; the newer technologies of shear-wave elastography and acoustic radiation force impulse (ARFI) imaging allow for quantification of tissue stiffness, enabling more precise tissue characterization, according to Beland.
"When applied to the liver, SWE has the potential to decrease the number of liver biopsies and offer a safer, more repeatable test to follow patients with liver disease," Beland said. "The technology is still being developed and the clinical applications such as liver disease need more study."
Several studies outside of the U.S. had found shear-wave elastography to be safe and effective for evaluating cirrhosis in hepatitis C patients and determined that real-time SWE was more accurate than transient elastography in staging fibrosis. However, questions still remain regarding the correlation of a focal area of liver assessed by SWE with the current reference standard of liver biopsy, according to the researchers.
Furthermore, the ability to estimate liver fibrosis noninvasively in a broader patient population beyond just hepatitis C patients would be advantageous, particularly with the growing incidence of nonalcoholic fatty liver disease, the group wrote (AJR, September, 2014, Vol. 203:3, pp. W267-W273).
As a result, the research team sought to determine the diagnostic accuracy of real-time SWE for assessing liver fibrosis in an unselected patient population of 50 individuals referred for clinically indicated random liver biopsy for diffuse liver disease. The researchers also wanted to assess the effect of steatosis on SWE, as prior studies had shown conflicting results on the correlation of SWE results and the degree of steatosis.
Of the 50 patients included in the study, 21 had hepatitis C. SWE was performed prior to patient biopsies using an Aixplorer system (SuperSonic Imagine) with an SC6-1 convex broadband probe. A subxyphoid approach was employed for one elastogram. With the patient in a supine or slight right anterior oblique position, two other elastograms were then acquired from the right lobe at two different craniocaudal locations. Measurements from SWE for the left lobe, right lobe (two), and biopsy location were compared with subsequent grading on pathology.
The researchers also analyzed steatosis and serum markers using multiple logistic regression, and they calculated optimized SWE thresholds using area-under-the-curve (AUC) analysis.
| Accuracy of SWE for predicting fibrosis | |||
| Biopsy site | Ipsilateral lobe | Contralateral lobe | |
| All patients | 0.85 (0.74-0.96)* | 0.89 (0.78-0.99) | 0.80 (0.67-0.93) |
| Hepatitis C patients | 0.82 (0.63-1.0) | 0.84 (0.67-1.0) | 0.59 (0.19-0.99) |
| Nonhepatitis C patients | 0.89 (0.75-1.0) | 0.88 (0.73-1.0) | 0.93 (0.89-1.0) |
The results indicate that real-time shear-wave elastography can accurately predict significant fibrosis (stage ≥ 2) in patients with and without hepatitis C, Beland said. Also, SWE measurements taken at the biopsy site or within the same lobe in hepatitis C patients may correlate better with pathologic staging than SWE measurements taken in the contralateral lobe from the biopsy site.
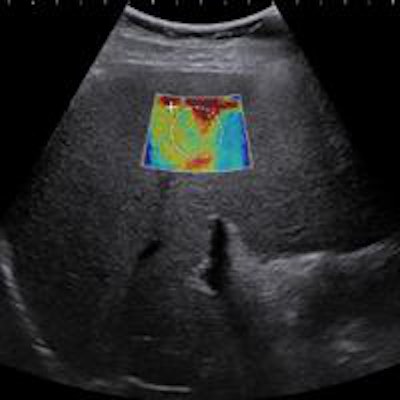
 Patient is a 48-year-old man with resolving acute steatohepatitis and cholestasis from alcohol intake with persistent ascites and abnormal liver function tests. Liver biopsy showed stage III fibrosis and 20% steatosis. Shear-wave elastography accurately predicted the presence of significant fibrosis with a shear-wave velocity of 2.83 m/sec at the biopsy site. Image courtesy of Dr. Michael Beland.
Patient is a 48-year-old man with resolving acute steatohepatitis and cholestasis from alcohol intake with persistent ascites and abnormal liver function tests. Liver biopsy showed stage III fibrosis and 20% steatosis. Shear-wave elastography accurately predicted the presence of significant fibrosis with a shear-wave velocity of 2.83 m/sec at the biopsy site. Image courtesy of Dr. Michael Beland.At the optimized biopsy site, SWE values for detecting Metavir score F2 or greater were 1.87 m/sec (75% sensitivity and specificity) for hepatitis C patients, 2 m/sec (80% sensitivity and specificity) in nonhepatitis C patients, and 1.89 m/sec (76% sensitivity and specificity) in all patients, the researchers calculated.
In other results, Beland said the group was "somewhat surprised to find no significant association between the presence and extent of steatosis with SWE values," nor did they find a correlation between SWE and various serum values typically associated with liver dysfunction.
Better than the standard?
Beland pointed out that it may be suboptimal to evaluate the accuracy of SWE by comparing it with the gold standard of liver biopsy. While a liver biopsy samples just 1/50,000 of the liver, liver disease -- particularly hepatitis C -- can be very heterogeneous in distribution.
"It may be that SWE can offer a more accurate picture of fibrosis than the biopsy, given the larger size of area measured and ability to do multiple measurements," he said.
In the next phase of research, Beland is actively developing new studies evaluating shear-wave elastography of the liver, as well as using ARFI imaging and SWE in the thyroid gland.


















