An ultrasound-based nomogram could help determine central cervical lymph node status in young patients diagnosed with thyroid cancer, according to research published online January 5 in Academic Radiology.
Researchers led by Yi Wei from Fudan University in Shanghai, China, found that their nomogram could accurately predict the negative status of papillary thyroid carcinoma by examining clinical and ultrasound features of central cervical lymph nodes.
"The nomogram could help predict the false positivity of unilateral clinically involved lymph node disease status, thus assisting clinicians in choosing better treatment strategies and maximizing patient benefits," Wei and colleagues wrote.
Previous research suggests that the incidence of thyroid cancer among people aged 30 and under is increasing, with papillary thyroid carcinoma being the main malignancy. Central cervical lymph node status is an important factor in disease prognosis.
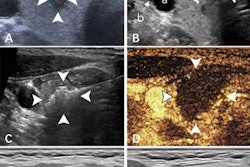
Ultrasound by itself is the preferred imaging method for this area, but some research has pointed out its variable accuracy. There are studies predicting central lymph node metastasis in node-negative patients; however, Wei and colleagues pointed out a lack of data on pathological lymph node negativity in unilateral clinically involved lymph node disease (cN1a) in papillary thyroid cancer patients.
Wei and colleagues wanted to look at the efficacy of a nomogram, a predictive graphical tool that uses both clinical and ultrasound features. They wanted to see if their nomogram could preoperatively predict negative nodal status of unilateral cN1a papillary thyroid cancer diagnosed in young patients. This could help predict false positives in patients with cancer diagnoses.
The team looked at data collected between 2016 and 2021 from 278 patients aged 30 and under. The youngest patients included were 13 years old. Out of the total, 21.2% were found to not have central lymph node metastasis pathologically.
After multivariate analysis, the following factors were independent predictors of metastasis: presence of Hashimoto's thyroiditis, T1 staging, no intratumoral microcalcification presence, and tumors located in the upper third of the thyroid gland.
The nomogram meanwhile showed promise in the training and validation cohorts, with areas under the receiving operator curve (AUC) of 0.764 and 0.728, respectively. The researchers also found high specificity for the nomogram in both cohorts.
| Performance of ultrasound-based nomogram in predicting central cervical lymph node status in young papillary thyroid cancer patients | ||
| Training cohort | Validation cohort | |
| Specificity | 83% | 83.3% |
| Sensitivity | 55.3% | 47.6% |
| Accuracy | 77.3% | 75.3% |
The nomogram has a zero- to 400-point scale that predicts nodal status. Total points are calculated by adding up points from ultrasound and clinical features, such as T staging, tumor location, and the presence of thyroiditis among others. The researchers found that a cutoff value of 220 points indicated probably nonmetastasis.
The study authors suggested that young patients with unilateral cN1a and who have a high possibility of pathological negative nodal status as predicted by the nomogram should be exempt from excessive cervical lymph node dissection.
However, they also called for more studies to improve the nomogram's accuracy. The authors wrote that this may be achievable by incorporating "more promising" features from updated technologies. These include elastography, contrast-enhanced ultrasound, and radiomics features among others.
"It is necessary to conduct further external validation in prospective multicenter studies with larger patient sizes," the researchers added. "The sensitivity is unfavorable, which may be attributed to the fact that only clinical and two-dimensional ultrasound features of the primary lesions were assessed in this study."