Ultrafast MRI may need to be reconsidered for classifying breast lesions, according to research published May 6 in Radiology.
A team led by Christiane Kuhl, MD, from University Hospital Aachen in Germany found that compared with 2D dynamic contrast-enhanced MRI (DCE-MRI), ultrafast MRI led to reduced lesion conspicuity and did not improve breast lesion calcification classification.
“Apparently, [2D] DCE-MRI with a temporal resolution of 60 seconds yields a similarly selective visualization of cancer versus noncancer as ultrafast MRI, but does not suffer from image degradation as heavily accelerated ultrafast imaging does,” the Kuhl team wrote.
Proponents of ultrafast breast MRI have highlighted the modality’s ability to boost lesion conspicuity, making lesions more distinguishable and defined on imaging. This addresses masking issues due to background parenchymal enhancement (BPE). Proponents also say this method improves classification of enhancing lesions.
But Kuhl and colleagues noted that published studies systematically penalized standard DCE-MRI. They explained that these studies integrated ultrafast MRI into existing DCE protocols, meaning postcontrast acquisitions of DCE-MR images began only after completion of ultrafast MRI.
The team compared the performance of both modalities intraindividually, where both were included in the precontrast phase. The study included a retrospective dataset of 31 women with a median age of 48 years, collected between 2021 and 2023. The women underwent DCE-MRI at 1.5 T and, within two days, a second contrast-enhanced exam using ultrafast MRI, for further diagnostic assessment. The team’s 2D DCE protocol offers a temporal resolution of 60 seconds per dynamic frame.
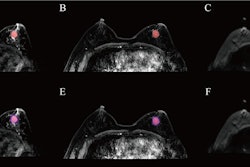
![Images depict axial MRI scans in a 50-year-old premenopausal female patient with biopsy-proven 12-mm invasive lobular cancer in the lower outer quadrant of the left breast. Upper images are subtracted dynamic contrast-enhanced (DCE) MRI scans from the first and second postcontrast acquisitions. Lower images are ultrafast MRI scans obtained within 24 hours after the DCE study (four consecutive subtracted dynamic frames from time points [T] 6–9). There is marked background parenchymal enhancement (BPE) on the DCE MRI scans. Thus, the known cancer (arrow) is barely visible; it exhibits only slightly stronger enhancement than the normal fibroglandular tissue, which results in low conspicuity. At ultrafast MRI there is less BPE, and still the cancer is barely visible because it starts to enhance simultaneously with the BPE. The conspicuity of the cancer is even reduced compared with the DCE series. Both of the readers missed this cancer on both the DCE and ultrafast MRI scans.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2025/05/2025-05-06-rsna-ultrafast-dce-mri-breast.Gzvq76udFr.jpg?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) Images depict axial MRI scans in a 50-year-old premenopausal female patient with biopsy-proven 12-mm invasive lobular cancer in the lower outer quadrant of the left breast. Upper images are subtracted dynamic contrast-enhanced (DCE) MRI scans from the first and second postcontrast acquisitions. Lower images are ultrafast MRI scans obtained within 24 hours after the DCE study (four consecutive subtracted dynamic frames from time points [T] 6–9). There is marked background parenchymal enhancement (BPE) on the DCE MRI scans. Thus, the known cancer (arrow) is barely visible; it exhibits only slightly stronger enhancement than the normal fibroglandular tissue, which results in low conspicuity. At ultrafast MRI there is less BPE, and still the cancer is barely visible because it starts to enhance simultaneously with the BPE. The conspicuity of the cancer is even reduced compared with the DCE series. Both of the readers missed this cancer on both the DCE and ultrafast MRI scans. RSNA
Images depict axial MRI scans in a 50-year-old premenopausal female patient with biopsy-proven 12-mm invasive lobular cancer in the lower outer quadrant of the left breast. Upper images are subtracted dynamic contrast-enhanced (DCE) MRI scans from the first and second postcontrast acquisitions. Lower images are ultrafast MRI scans obtained within 24 hours after the DCE study (four consecutive subtracted dynamic frames from time points [T] 6–9). There is marked background parenchymal enhancement (BPE) on the DCE MRI scans. Thus, the known cancer (arrow) is barely visible; it exhibits only slightly stronger enhancement than the normal fibroglandular tissue, which results in low conspicuity. At ultrafast MRI there is less BPE, and still the cancer is barely visible because it starts to enhance simultaneously with the BPE. The conspicuity of the cancer is even reduced compared with the DCE series. Both of the readers missed this cancer on both the DCE and ultrafast MRI scans. RSNA
The team reported 59 enhancing lesions in the 62 breasts included in the study. While ultrafast MRI led to lower BPE ratings, it did not outperform DCE-MRI in terms of lesion conspicuity and image quality as independently rated by two breast radiologists.
Comparison between ultrafast MRI, DCE-MRI | |||
Measure (average) | DCE-MRI | Ultrafast MRI | p-value |
BPE rating | 3.3 | 2.5 | < 0.001 |
Lesion conspicuity | 4.1 | 3.5 | 0.001 |
Image quality | 4.1 | 2.3 | < 0.001 |
The researchers also reported that ultrafast MRI did not lead to more assessable lesion morphology, including shape, margin, and internal architecture (p < 0.05 for all). And kinetic parameters derived from ultrafast MRI did not improve enhancing lesion classification when compared to parameters derived from DCE-MRI.
At ultrafast MRI, time to enhancement was shorter for malignant versus benign lesions (p = 0.01). However, the maximum slope did not differ. Meanwhile, for DCE-MRI, both the wash-in rate and time course pattern significantly differed between malignant and benign lesions (both p = 0.01).
The study authors highlighted that their results should bring on more research on the best compromises between spatial versus temporal resolution to make more evidence-based recommendations for DCE-MRI.
The results provide necessary direct data on ultrafast MRI’s limitations, according to an accompanying editorial written by Claudia Cotes, MD, and Michael A. Jacobs, PhD, from the University of Texas Health Science Center in Houston.
“Although the authors of previous studies have advocated for ultrafast imaging due to its speed and accessibility, this new research highlights the potential important diagnostic compromises involved and indicates that further studies are needed to determine the optimal role of [ultrafast breast] MRI, particularly to find the ideal balance between efficiency and diagnostic reliability in breast imaging,” they wrote.
The full study can be found here.














![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)

