After years of gaining clinical approval, computer-aided detection (CAD) for mammography has hit a rough patch of late, with insurance payors like UnitedHealthcare of Minneapolis and ODS Companies of Portland pondering cuts to CAD reimbursement. The question for insurers and also clinicians is whether CAD is effective in detecting more cancers.
Boston researchers addressed this issue in a study published in the American Journal of Roentgenology. Dr. Dianne Georgian-Smith and colleagues from the department of radiology and breast imaging at Brigham and Women's Hospital, the Avon Breast Center, and the department of radiology at Massachusetts General Hospital compared a human second reader of screening mammograms with CAD for reducing false-negative cases by a primary radiologist (AJR, November 2007, Vol. 189:5, pp. 1135-1141).
They found that both a human second reader and the use of CAD can increase the cancer detection rate.
The study included 6,381 consecutive screening mammograms taken between June 2001 and April 2003 at one outpatient screening center using a film-screen unit. The studies were scanned using a CAD system. Eight academic breast imagers independently reviewed these mammograms. None of them reviewed a dominant number of the study sample; the mean percentage of cases per radiologist was 12%; and the interpretations represented a cross section of the practice so that the results could be generalized.
The primary radiologist read the mammogram alone, then read the CAD results; a second reader, different from the primary radiologist, then looked for areas of suspicion on the images, without knowledge of the CAD results but with knowledge of the primary reader's results. Clinical care was based on the results of both the CAD and the second radiologist reads.
The primary reader called back 475 of the 6,381 cases (7.4%). Biopsies were suggested in 70 of these 475 cases (14.7%). Of these 70 biopsied cases, 13 malignancies were found (18.6%) for a primary reader screening detection rate of 2.04 cases per 1,000 women.
An additional 30 cases were called back by the CAD reader, for a callback rate of 0.47% cases. Of these 30 callbacks, three were recommended for biopsy. None of these three was malignant.
The second human reader called back 34 cases in addition to the primary reader's callbacks. Except for one, these callbacks were different from the CAD-marked callbacks. Five of these 34 cases were recommended for biopsy; two (40%) were malignant. The CAD system had marked these two lesions, but the primary reader had dismissed them.
 |
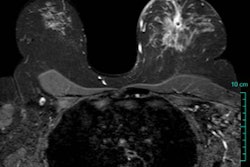
| False-negative case for all reviewers: 76-year-old woman with invasive ductal carcinoma. Above, craniocaudal mammogram obtained four years before study in which mass (arrow) was excised and was found to be benign (fibrocystic changes without atypia) at histology. Middle, screening mammogram, craniocaudal view, two years before study shows postsurgical changes. Below, screening mammogram, craniocaudal view, at time of study in which increase in density at biopsy site was not detected by any of reviewers, although area was marked by CAD system. |
 |
 |
| Georgian-Smith D, Moore RH, Halpern E, Yeh ED, Rafferty EA, D'Alessandro HA, Staffa M, Hall DA, McCarthy KA, and Kopans DB, "Blinded Comparison of Computer-Aided Detection with Human Second Reading in Screening Mammography" (AJR 2007; 189:1135-1141). |
The second reader increased the cancer detection rate from 13 by the primary reader to 15, for a relative increase in the cancer detection rate of 15.4%. The overall screening cancer detection rate for all three readers was 2.35 per 1,000 women; three malignancies were not found by any of the readers but developed within one year, bringing the total of cancers in the study to 18 during the time of imaging.
The study showed that a CAD system and a human second reader's results weren't statistically significantly different as measured by malignancy detection rates or callback rates, as both CAD and the second reader added cases to those the primary reader had identified. Georgian-Smith acknowledged that the study sample was too small to show whether the CAD read or second human read was superior. Rather, the data highlighted a key issue when it comes to CAD: the technology can find a lesion, but the human reader still has to determine its meaning and significance.
A second human reader may have the edge over CAD because that second reader may have a different interpretation of the findings compared to the primary radiologist, which can lead to earlier diagnosis, and a human reader can ascribe significance to suspicious areas, while a CAD system simply marks them.
The study showed reader variability between the two human readers: Of the 64 cases called back by the CAD reader and the second human reader, only one case was called back by both. The two forms of double reading may look the same statistically, but may be dramatically different, Georgian-Smith wrote.
To show statistical significance between a human second reader and the CAD reading, a study would need more than 24,000 screening cases, and all the cancers would have to be identified by only one reader, which isn't feasible, the researchers concluded. In addition, the fact that the CAD system was used on film-screen exams, rather than digital ones, might affect the study results.
CAD can minimize perceptual failure, but can't compensate for interpretation failure, Georgian-Smith wrote. A second human reader can offer a second interpretation and an increase in perception, although for many facilities, especially those using digital mammography, adding a second human read to the workflow can be challenging.
By Kate Madden Yee
AuntMinnie.com contributing writer
November 16, 2007
Related Reading
UnitedHealthcare ponders cuts to CAD reimbursement, October 26, 2007
CAD still not out of the woods, despite Oregon payor's reversal, July 24, 2007
Oregon payor reverses stand, reinstates CAD payments, July 23, 2007
NEJM study prompts Oregon payor to cancel CAD reimbursement, July 11, 2007
Studies show CAD matches up well with CR mammo, FFDM, May 24, 2007
NEJM study pans CAD, draws attention and criticism, April 5, 2007
Copyright © 2007 AuntMinnie.com