In results that could potentially shake up the heart imaging status quo, a machine learning algorithm slightly outperformed a more traditional algorithm in analyzing fractional flow reserve CT (FFR-CT) studies for detecting signs of ischemic coronary lesions, according to a presentation at the recent RSNA 2016 meeting in Chicago.
Researchers from the Medical University of South Carolina (MUSC), Yale University, and the University of Frankfurt Medical Center and University of Munich in Germany compared two algorithms for their ability to detect ischemic lesions in patients undergoing coronary CT angiography (CCTA) and other tests for coronary artery disease. One was a traditional FFR-CT approach that analyzes CCTA scans based on geometric patterns in the images, while the other was a machine learning approach to computational flow dynamics.
While both algorithms were superior to CCTA and invasive angiography, the machine learning algorithm provided greater specificity than the traditional approach on a per-lesion basis, and it also had a higher positive predictive value, said Dr. Moritz Albrecht, a research fellow at MUSC, in a presentation at the conference. When analyzed by patient, machine learning was found to boost sensitivity, specificity, and positive and negative predictive values.
Determining lesion significance
CCTA has a proven track record in ruling out coronary artery disease; however, by itself, it cannot confirm whether a detected coronary artery stenosis is significantly limiting blood flow. This means that patients with stenosis of 50% to 70% at CCTA must undergo additional functional testing such as SPECT myocardial perfusion or, increasingly, FFR-CT if they are to avoid having an invasive coronary angiography with the potential of revealing no ischemic coronary disease.
 Dr. Moritz Albrecht from MUSC.
Dr. Moritz Albrecht from MUSC.Machine learning solutions are on the rise in radiology for their ability to learn patterns in medical images that are characteristic of disease. At the same time, fractional flow reserve CT is a proven technique for analyzing flow patterns in the coronary arteries to determine the significance of coronary artery lesions.
Based on this information, the researchers decided they wanted to see how well a machine learning approach to FFR-CT analysis, which they called cFFRML, compared with a more traditional FFR-CT approach based on analysis of computational flow dynamics (cFFRCFD).
The cFFRCFD algorithm, a research prototype from Siemens Healthineers, is based on a coronary artery model with patient-specific boundary conditions including blood pressure, heart rate, and left ventricular mass, per research by Itu et al. Meanwhile, the cFFRML algorithm uses a deep learning framework to compute the functional severity of lesions; it is trained to utilize a large database of synthetically generated coronary anatomies and their corresponding homodynamic conditions from a computational fluid dynamics simulation.
Albrecht and colleagues compared the performance of both techniques on a per-lesion and per-patient basis. They also visually graded stenoses on CCTA, invasive coronary angiography, and invasive fractional flow reserve as the gold standard.
Machine learning's advantage
On a per-patient basis, both FFR-CT algorithms "were superior in sensitivity to CCTA and invasive angiography, but the cFFRML algorithm provided slightly higher parameters compared to the cFFRCFD algorithm for all measures: sensitivity, specificity, and positive and negative predictive values," Albrecht said.
| Comparison of algorithms for FFR-CT analysis on per-patient basis | ||||
| Parameter | CCTA | Quantitative coronary angiography | cFFRCFD | cFFRML |
| Sensitivity | 91% | 74% | 85% | 87% |
| Specificity | 33% | 82% | 88% | 89% |
| Positive predictive value | 41% | 45% | 80% | 82% |
| Negative predictive value | 86% | 88% | 91% | 92% |
On a per-lesion basis, the machine learning algorithm delivered the same sensitivity as traditional fractional flow reserve (77%), but the machine learning algorithm's specificity was a little higher, at 96% versus 94% for fractional flow reserve. Even so, the per-lesion analysis revealed no differences in accuracy between the two algorithms, Albrecht said.
Additionally, a Bland-Altman analysis showed no systemic bias, with a mean difference value for both cFFRML and cFFRCFD of 0.003. The Pearson's correlation coefficient for both cFFRML and cFFRCFD with invasive FFR was r = 0.68 (p < 0.0001).
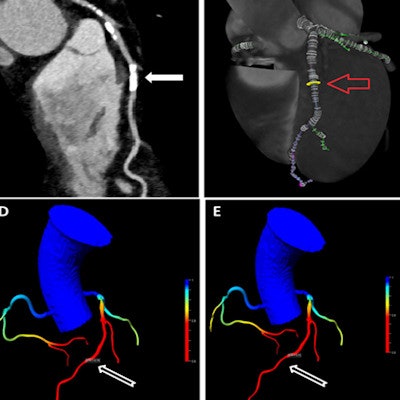
 In a 53-year-old man with chest pain, both CCTA and invasive coronary angiography showed 50% stenosis of the middle left anterior descending (LAD) artery, while cFFRML and cFFRCFD showed a greater degree of stenosis, at 74% and 73%, respectively. Image courtesy of Dr. Moritz Albrecht.
In a 53-year-old man with chest pain, both CCTA and invasive coronary angiography showed 50% stenosis of the middle left anterior descending (LAD) artery, while cFFRML and cFFRCFD showed a greater degree of stenosis, at 74% and 73%, respectively. Image courtesy of Dr. Moritz Albrecht.Both algorithms performed better than CCTA and quantitative coronary angiography (p < 0.04); however, there were no significant differences between cFFRML and cFFRCFD receiver operating characteristic (ROC) curves (p < 0.95).
Albrecht noted several limitations of the study, including the relatively small cohort of 58 patients, the study's single-center design, and its small number of positive cases. Finally, no patients with stents, coronary artery bypass grafts (CABG), or cardiac devices were enrolled.
The machine learning algorithm "enables incorporation of information extending beyond lumen geometry," he said.
The algorithm may enable the comprehensive integration of information regarding coronary plaque, including plaque type, total plaque burden, and positive remodeling, which are not components of current computational fluid dynamics algorithms, Albrecht concluded.