GENEVA - Japanese researchers hope to supplant the invasive and time-consuming process of diagnosing Crohn's disease with a CT technique that is unaffected by intestinal stenosis and other impediments to conventional endoscopic evaluation.
Their work, presented at the 2010 Computer Assisted Radiology and Surgery (CARS) meeting, uses advanced imaging processing to highlight subtle depressions in the mucosa of the small intestine that represent intestinal ulcers.
"Crohn's disease is an inflammatory disease of the digestive tract [affecting] increasing numbers of patients in Japan," said Masahiro Oda from Nagoya University's MEXT Innovative Research Center for Preventive Medical Engineering in Nagoya. Found in both the small and large intestines, Crohn's disease is characterized by "intestinal stenoses and longitudinal ulcers," he said.
Conventional diagnosis of Crohn's is a protracted process that often begins with stool and antibody tests to rule out other inflammatory bowel diseases, eventually leading to optical or capsule endoscopy, which allows the physician to assess the extent and location of inflammatory damage to the intestinal wall.
"Diagnosis takes a long time -- several hours -- and it is difficult to perform diagnosis of the whole intestine because endoscopes cannot pass through intestinal stenoses," Oda said.
Oda, along with colleagues including Kensaku Mori, PhD, and Kazuhiro Furukawa, proposed an automated CT computer-aided detection (CAD) system that would be minimally invasive and would make it possible to observe the whole intestine irrespective of intestinal stenosis.
Although both CT and MRI have been used previously to diagnose Crohn's, radiologists have found it "difficult to find the lesions and understand the complicated shapes of large and small intestines," Oda said. "Easy-to-observe visualization and automated lesion detection are important for diagnosis."
CAD can detect concave regions in the digestive tract caused by longitudinal ulcers, Oda said. The proposed method relies on a local intensity structure analysis method for automated detection of concave regions.
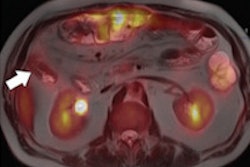
The CAD system displays five views of the intestine simultaneously, including a virtual unfolded view, virtual endoscopic view, curved planar reconstruction view, multiplanar reconstruction view, and the outside wall of the intestine, Oda said.
The display indicates intestinal stenosis by changing the height of the virtual unfolded view, and it enhances longitudinal ulcers via concave region enhancement, Oda said.
 |
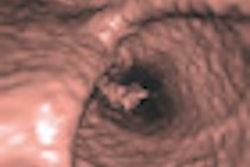
| Virtual endoscopy display shows five different views of the intestinal tract on a single screenshot, including (clockwise from top) virtual unfolded view, curved planar reconstruction view, multiplanar reconstruction view, outside view, and virtual endoscopy view. Unfolded view (top arrow) shows stenotic narrowing, which is further characterized by curved planar reconstruction (middle arrow) and virtual endoscopy (bottom arrow) views. All images courtesy of Masahiro Oda. |
During preprocessing, the inner regions of the small and large intestines are extracted from a fecal-tagged 3D CT image. Air-filled regions are then subtracted using thresholding of the CT data, which is followed by a region-growing process. Small unconnected components of the intestine as well as lung tissue are subtracted during this process. Regions of tagged fluid are removed using an electronic cleansing method, Oda said.
The system finds concave regions of the intestinal mucosa by looking for changes in CT attenuation values, which "tend to gradually decrease from outside of the concave region to inside of it," Oda said. "We used the inverse-blob structure enhancement filter designed to detect colonic polyps surrounded by tagged fluid to detect concave regions on the intestinal wall."
 |
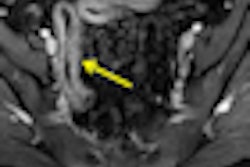
| Slide describes concave region enhancement (CRE) technique (above) targeting hollow regions on intestinal wall caused by longitudinal ulcers. |
Thresholding of CT values was used for false-positive reduction, and the system eliminated other false positives by removing small, isolated groups of voxels that met the CT threshold criteria but would not have represented ulcerative depressions, Oda said.
All CT images were acquired using a 512 x 512-pixel field-of-view and 0.5-mm slices.
"We observed the intestines of 11 fecal-tagging abdominal CT images using the system," he said. "Changing the height of virtual unfolded views enabled intuitive understanding of positions of intestinal stenosis. In addition, the virtual endoscopy, curved planar reconstruction, and multiplanar views permitted close inspection of the intestinal wall."
As an adjunct to stenosis detection, concave region enhancement (CRE) in blue enables efficient diagnosis of longitudinal ulcers, according to Oda. "However, CRE generated a lot of false positives," he said. Bubbles on the fluid surface inside the intestinal lumen and the base of haustral folds were the two most frequent sources of false positives.

Future work will focus on the concentration ratios of concave regions along the intestinal mucosa as a target for developing more sophisticated techniques to reduce false positives, he said.
A further limitation of the system was seen in the outside view, which was difficult to evaluate in regions that had many overlapping intestinal loops. Selective display of the intestine will be key to improving functionality in this view, Oda said.
The team plans to focus on improving the performance of concave region detection and on adding functions that highlight other common indicators of Crohn's disease. In response to a question from the audience, Oda said it is difficult to segment completely stenosed regions of the intestine.
By Eric Barnes
AuntMinnie.com staff writer
June 29, 2010
Related Reading
ASIR halves VC dose without drop in image quality, June 21, 2010
Capsule endoscopy useful, safe in children, May 28, 2010
CT shows abdominal fat is unreliable Crohn's treatment target, April 14, 2010
MRI enterography shows shortcomings for Crohn's disease, February 23, 2010
ASIR cuts dose in Crohn's disease patients, December 4, 2009
Copyright © 2010 AuntMinnie.com