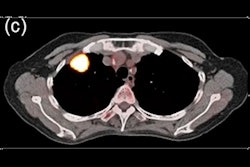
A nomogram based on radiomics features and clinical variables can help to identify an uncommon form of lung cancer that mimics the appearance of pneumonia on CT, according to research published September 14 in the American Journal of Roentgenology.
A team of researchers led by Xinxin Yu, PhD, of Shandong University in China found that the combined nomogram yielded better results than a model based only on clinical variables for the difficult task of distinguishing between pneumonia and pneumonia-type invasive mucinous adenocarcinoma (IMA). What's more, it also outperformed two cardiothoracic radiologists.
"The findings support potential clinical use of the nomogram for diagnosing pneumonia-type IMA in patients with consolidation on chest CT," the authors wrote.
Invasive mucinous adenocarcinoma accounts for up to 5% of lung adenocarcinoma cases. The pneumonia type accounts for 8.2% of IMA cases and has a worse prognosis than the solitary type of IMA. However, pneumonia-type IMA has a similar appearance on CT to pneumonia, as well as overlapping clinical manifestations. Consequently, it's often misdiagnosed as pneumonia, according to the researchers.
Although it's critical to differentiate pneumonia-type IMA and pneumonia in order to provide appropriate early treatment, identification of pneumonia-type IMA on CT in clinical practice currently depends on the radiologist's judgment and experience, according to the researchers.
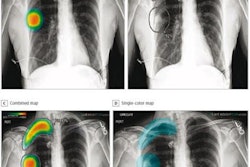
To help address this diagnostic challenge, the researchers sought to develop a nomogram that combined clinical and radiomics features for diagnosis of pneumonia-type invasive mucinous adenocarcinoma. They first gathered a total of 314 patients from six hospitals who had received a noncontrast-enhanced CT scan showing consolidation. Of these, 106 were diagnosed with pneumonia-type IMA and 208 had pneumonia.
The researchers trained and validated the clinical model, radiomics signature, and a nomogram incorporating both clinical variables and radiomics features from a dataset of 245 patients from three hospitals. The 69 patients from the three other hospitals served as the external test set.
They winnowed the list of 1,743 radiomics features that were initially extracted from the images down to a final radiomics "signature" of 15 features. The authors also developed a clinical model using the only two clinical variables independently predictive of pneumonia-type IMA: absence of fever and family history of lung cancer.
Next, they compared the performance of the clinical model and the combined nomogram with two cardiothoracic radiologists with seven and 14 years of postraining experience, respectively.
Decision-curve analysis revealed that the combined nomogram offered a higher overall net benefit than from the clinical model on the external test set. The combined nomogram also yielded better results than the two radiologists.
| Improved detection of pneumonia-type IMA from CT radiomics/clinical nomogram | |||||
| Radiologist 1 | Radiologist 2 | Clinical model | Radiomics signature | CT radiomics and clinical variables model | |
| Area under the curve | 0.7 | 0.67 | 0.71 | 0.81 | 0.85 |
The difference between the combined model and the clinical model were statistically significant (p = 0.01).
Delving further into the results, the combined nomogram produced 46.9% sensitivity, 94.6% specificity, and 72.5% accuracy on the external test set. Given its uncommon nature, the model's high specificity for pneumonia-type IMA may be of greater priority, though, than the low sensitivity, according to the researchers.