Readers using an original computer-aided detection (CAD) algorithm that subtracts thoracic 3D CT images from follow-up images found more vertebral metastases than readers working unaided, according to a study in PLOS One.
The software could aid in the early detection of vertebral metastases that are common and potentially harmful in lung cancer patients, the investigators said.
"Our temporal 3D CT subtraction CAD software easily detected vertebral metastases on the follow-up CT images of lung cancer patients regardless of the osteolytic or osteoblastic nature of the lesions," wrote Dr. Shingo Iwano and colleagues from Nagoya University in Japan and Fujifilm (PLOS One, January 17, 2017).
Common problem, inadequate solutions
Bone metastases occur in 10% to 40% of patients during or after primary lung cancer treatment, with the spine being the most common site, the authors noted. These metastases are responsible for a litany of problems, including pain progression, compression fractures, and neural disturbances, making early detection critical.
MRI and PET are the most common imaging techniques for detecting metastases; however, neither modality is part of the routine follow-up for lung cancer patients, according to the authors. CT, on the other hand, is used routinely to check for local recurrence and metastases in lung cancer patients, although it is less sensitive than PET and MRI for detecting vertebral metastases.
At CT, osteolytic masses show lower attenuation than surrounding bone, while the attenuation of osteoblastic metastases is higher. Using CAD to detect vertebral metastases is challenging due to these attenuation differences and other factors. However, recent reports show that temporal subtraction chest 3D CT can detect both osteolytic and osteoblastic lesions.
"We have developed an original CAD software that can subtract the follow-up and initial 3D CT of the spine with the application of the nonrigid registration," the authors wrote.
CAD detection in 30 cases
In the study, DICOM data of chest CT scans were transferred to a workstation on which the group's own CAD software was installed. Sagittal and coronal multiplanar reconstruction (MPR) images from continuous thin-section CT images were automatically displayed on the workstation, with follow-up images on the left half of the monitor and initial images on the right half to enable easy visual comparison.
The reading test involved 30 randomly selected digital chest CT images. Cases were extracted from the facility's PACS based on searches for "spine," "bone metastasis," and "lung cancer," and they were reviewed by an experienced chest radiologist who selected 15 cases with new-onset bone metastasis during lung cancer follow-up. An additional 15 cases without bone metastases were collected. Except for the presence of metastasis, there were no significant differences between the two groups.
The CAD software works as follows:
- First, it detects the centerline of the spine at initial and follow-up CT. CAD detects highly deformed vertebrae as compression fractures, and if one is detected, an alert is rendered on the monitor to caution against misregistration by 3D CT subtraction, the authors explained.
- Next, 3D template matching along the centerline is used to determine the corresponding vertebra between the initial and follow-up images. 3D CT subtraction is then performed using nonrigid deformation.
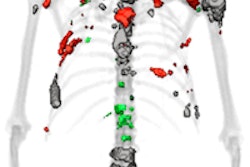
- Finally, the color-coded difference of the 3D model is superimposed on the follow-up monochromatic MPR images. Osteolytic lesions (blue) and osteoblastic lesions (red) are color-coded. The case below shows vertebral metastases diagnosed by the CAD software.
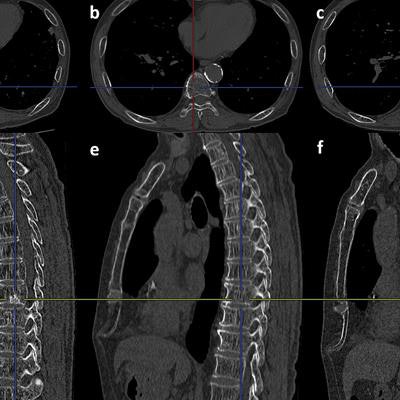
 A case of osteoblastic metastasis in the body of the ninth thoracic vertebra. (a) Follow-up axial image. (b) Initial axial image. (c) Result of the 3D CT subtraction. The blue color indicates the metastasis. (d) Follow-up sagittal image. (e) Initial sagittal image. (f) Result of the 3D CT subtraction. The blue color indicates the metastasis. Image republished courtesy of PLOS One, January 17, 2016.
A case of osteoblastic metastasis in the body of the ninth thoracic vertebra. (a) Follow-up axial image. (b) Initial axial image. (c) Result of the 3D CT subtraction. The blue color indicates the metastasis. (d) Follow-up sagittal image. (e) Initial sagittal image. (f) Result of the 3D CT subtraction. The blue color indicates the metastasis. Image republished courtesy of PLOS One, January 17, 2016.Improvement for all readers, lesion types
According to the results, both readers detected greater numbers of both types of lesions -- and greater numbers of true positives -- with CAD than without it.
"Our temporal 3D CT subtraction CAD software easily detected vertebral metastases on the follow-up CT images of lung cancer patients regardless of the osteolytic or osteoblastic nature of the lesions," during routine interpretation of a thoracic CT image for follow-up of primary lung cancer, Iwano and colleagues wrote.


The detection of vertebral metastases with and without CAD. Image republished courtesy of PLOS One, January 17, 2016.
The total reading time for reader A was 1 hour, 41 minutes (3.4 min per case), and for B it was 1 hour, 50 minutes (3.7 min per case), the group wrote. The kappa statistic showed good reproducibility between the readers for assessments without CAD (0.672, p < 0.001) and with CAD (0.651, p < 0.001).
The detection of metastases by both readers improved more in the posterior component using CAD than without CAD, possibly due to the difference in the 3D form between the vertebral body as anterior components and posterior components, the authors wrote.
The CAD software was designed to emphasize the results of bone subtraction by adding color to the monochromatic CT images. Color could also be used to distinguish between osteolytic lesions, shown in red and yellow, and osteoblastic lesions, shown in blue.
"Because osteolytic vertebral metastases cause pathological fractures more often than osteoblastic ones, differential diagnosis between them is important," Iwano and colleagues wrote.
Detection is paramount
Bone metastases cause a range of problems including skeletal-related events requiring radiotherapy or surgery, as well as pathological fractures and spinal cord compression, which can cause severe pain, paralysis, gait disturbance, and bladder and rectal disturbance.
"These complications cause significant morbidity and reduced [quality of life]," the authors wrote. "Therefore, it is important for the physician and radiologist not to overlook them in routine checkup imaging even if a patient has no symptoms."
Limitations of the study included its retrospective nature and single-center design, they noted. However, the temporal subtraction 3D CT software readily detected vertebral metastases on follow-up CT images of lung cancer patients, the authors concluded.
"This software could prevent radiologists from overlooking asymptomatic vertebral metastases during routine interpretation of thoracic CT images for follow-up of lung cancer," Iwano and colleagues wrote.