CHICAGO - A state program using a clinical decision-support tool was described modestly today at the first scientific session on informatics. However, assuming that the statewide rollout is as successful as a pilot project that involved half of Minnesota's insured population, it may someday be regarded as a pioneer in informatics practice-change, with both national and global implications.
Cally Vinz, vice president of clinical products and strategy of the Institute for Clinical Systems Improvement (ICSI) in Bloomington, MN, described how the overwhelming success of a pilot program launched in 2007 to reduce overuse of high-technology diagnostic imaging exams is expanding into a statewide initiative throughout Minnesota in 2011.
On November 10, ICSI announced that it was offering free use of the clinical decision-support tool to every healthcare provider in the state. Decision-support assistance with respect to ordering CT, MRI, PET, and nuclear cardiology exams is being extended to virtually every person living in the state, including the uninsured and Medicare/Medicaid patients.
What's even more impressive is that the participating Minnesota health insurance companies are footing the bill and underwriting the cost of the software (RadPort, Nuance Communications, Burlington, MA).
How the project began
Beginning in 2003, utilization of high-tech imaging exams had been steadily increasing at an annual rate of 8%. Alarmed by this steady increase -- and concerned that the cost would be unsustainable -- the Minnesota Legislature mandated that preauthorization programs be implemented to validate diagnostic appropriateness of these exams and maintain exam affordability for its public program participants.
Two options were available to comply with the new law: utilize the services of radiology benefits management (RBM) companies or voluntarily comply with evidence-based guidelines for these exams. Some healthcare providers who had been using RBMs complained that they were expensive and inefficient. The process of obtaining approval could be slow and cumbersome. Scheduling of exams that were ultimately authorized was often delayed, and time spent by clerical and clinical staff on the process was extensive and expensive to the provider, Vinz explained.
Seeking a better solution, major health insurance companies and five large healthcare organizations requested that ICSI develop a patient-centric and efficient way to achieve the state's mandate. Collectively, these organizations provided healthcare services to approximately half of the insured population in the state.
Payors and providers in Minnesota have a culture of being collaborative and consensus-driven, Vinz explained. They were willing to work together to develop a solution that would benefit everyone.
A steering committee was developed to design a one-year pilot program to determine if medical groups could use standardized appropriateness criteria based on the American College of Radiology (ACR) and other specialty organizations to order CT, MRI, PET, and nuclear cardiology exams while with the patient.
The primary goal of the pilot program was to improve the appropriateness of imaging orders, as well as provide rapid and easily understood feedback to clinicians to help them order the best test for the patient. Patients and their physicians were to have immediate access to the best clinical science available.
Other goals included establishing outcomes reporting to correlate report findings with ICD9 codes and exam types, developing internal quality improvement efforts based on utilization and appropriateness data, auditing and analyzing results to drive further improvements, and using this data to expand or revise the appropriateness criteria.
The pilot program participants included five large medical groups, four health insurance companies, a large radiology practice, and the Minnesota Department of Human Services.
More than 2,300 providers agreed to use appropriateness criteria when ordering any of the top 90% of CT, MRI, PET, and nuclear cardiology exams. The appropriateness criteria was either embedded into the organizations' electronic medical record (EMR) systems (Epic Systems, Verona, WI) or could be accessed through the Internet using an ICSI managed Web portal.
First-year accomplishments
During 2007, the program's participants submitted approximately 47% of the claims to the four major Minnesota health plans, whose companies were participants in the pilot. The remaining 53% of the claims were filed by hospitals and medical groups using the services of RBMs.
The combined effort of both groups decreased by 3% the number of claims for the targeted exams in 2007, when compared to 2006. The leveling off to 0% growth in 2007 was estimated to have saved almost $60 million, Vinz reported. Approximately $28 million was attributed to the decision-support approach.
Additionally, an audit at one medical group had been conducted to evaluate how clinical decision support may have affected the diagnostic appropriateness of exams ordered. Six hundred charts of patients who had undergone head CT, head MRI, and lumbar spine MRI exams were randomly selected. Half represented exams performed six months before the clinical decision-support tool was available, and half were performed six months after implementation.
The audit revealed that using the clinical decision-support tool had increased diagnostic quality by approximately 10%. When the tool was used, 89.2% of the exams had been appropriately ordered, compared to 79.5% for the other group.
All participants in the pilot project agreed to continue using the system. During calendar years 2007 through 2009, more than 1 million high-tech exams were ordered by physicians of the five medical groups, saving Minnesota an estimated $84 million.
"Both patients and their physicians overwhelmingly appreciated the clinical decision-support system," Vinz said. "They could see the evidence-based recommendations of what exams were most appropriate, schedule an exam on the spot, and not experience any surprises or delays."
"Radiologists were as supportive of the system as the ordering physicians," she said. "They felt that their expertise was better used consulting with ordering physicians about complex cases."
Everyone involved appreciated the efficiency of the system, which translated directly as cost savings to both providers and payors, according to Vinz. Fairview Health Services, which ordered an average of 1,850 high-tech diagnostic imaging exams per month, reduced its clerical cost related to preauthorization from 10 minutes to 10 seconds per exam, on average. The medical group reported to ICSI that one month it had spent 308 hours to obtain RBM approval, but by substituting decision support, ordering a comparable number of scans took an average of five hours per month. Over the past three years, Fairview has saved 11,000 hours in administrative time.
ICSI began with a self-developed system, but it quickly recognized that adopting a commercial clinical decision-support system was advantageous. "The absolute beauty of this system is that keeping current and updated with appropriateness criteria is managed through a process by the vendor," Vinz said. "Each EMR reaches to a central server, and for healthcare providers who don't have an EMR or don't have an EMR for which we currently offer an interface, if they can access the Internet, they can log onto the decision-support Web portal in real-time."
If a provider wants to override the clinical decision-support recommendation, he or she can do so, and if a health insurance plan incorporates a modification or exception, the system will post a special notification. "But if you develop your own criteria, you have no consistency, and we believe that everyone participating in this program supports the power of consensus," Vinz told AuntMinnie.com in an interview.
 |
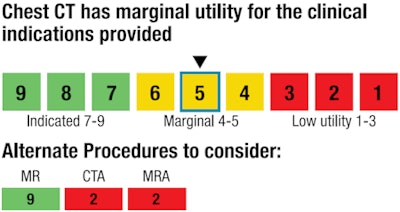
| Sample response from the clinical decision-support system. Image courtesy of ICSI. |
What's next
In essence, this program is the pilot for a $10 million decision-support demonstration project that the Centers for Medicare and Medicaid Services (CMS) is funding. Vinz said that ICSI did not apply to participate in the program because the state's endeavor is way ahead of what CMS intends to do. In fact, CMS representatives consulted with the three-person ICSI program management team in June 2010.
ICSI is gathering data and eventually will be able to show ordering rates, utilization rates, different ordering patterns by healthcare provider groups, and outlier information. By 2012, it hopes to perform sophisticated analysis that will be able to improve the Minnesota healthcare community's knowledge of which diagnostic tests result in the best patient outcomes based on different conditions, Vinz said.
Meanwhile, individual healthcare providers can purchase a data warehouse tool (RadCube, Nuance) that collates radiology orders with radiology reports for deep analysis of ordering trends and patient outcomes.
By Cynthia E. Keen
AuntMinnie.com staff writer
November 28, 2010
Related Reading
CMS unveils imaging decision-support initiative, July 23, 2010
One-quarter of outpatient CT and MRI exams are inappropriate, March 1, 2010
CDC report: MRI, CT, PET use spikes in physician offices, ER, February 18, 2010
ACR lobbies against RBMs, utilization rate changes, June 26, 2009
ACR, others form Imaging e-Ordering Coalition, June 16, 2009
Copyright © 2010 AuntMinnie.com


















