A new study published online July 30 in the Journal of the National Cancer Institute indicates that the use of advanced imaging is growing faster among patients with stage IV cancer than it is among patients with earlier stages of disease. The findings could mean that imaging is being overused in terminally ill patients.
The study found that the proportion of stage IV cancer patients who received advanced imaging grew nearly 5% among a sample Medicare population, while falling more than 2% among those with early-stage cancer. What's more, more than one-third of patients were scanned in their last month of life.
The results indicate that better clinical guidelines are needed regarding the use of imaging in patients with advanced disease, according to both the study's authors and an independent commentary.
Rising Medicare costs
The study notes that more than 25% of Medicare dollars are spent on patients at the end of their lives. In addition, the annualized net costs of cancer are highest in the last year of life, and care delivered during this time is intensifying, according to the research group from the Dana-Farber/Harvard Cancer Center, Brigham and Women's Hospital, and the University of Wisconsin. The lead author of the study was Dr. Yue-Yung Hu from Brigham and Women's (JNCI, July 30, 2012).
Little is known about imaging use in cancer patients at the end of their lives, according to the authors, so they decided to track advanced imaging in patients with breast, colorectal, lung, or prostate cancer, which represent the four most common causes of death from cancer. They defined advanced imaging as CT, MRI, nuclear medicine, PET/CT, and PET.
The group analyzed imaging trends and frequency of exams in 105,594 Medicare patients diagnosed with stage IV cancer between 1995 and 2006, drawn from the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) cancer registry. From this cohort, the researchers created a subgroup of 55,253 patients who had been diagnosed during calendar years 2002 through 2006 to serve as the "recent care" group.
For comparison purposes, Hu and colleagues expanded the study population to include patients diagnosed with stage I or stage II disease of the same four tumor types between 1995 and 2006, for a total population of 192,429 patients. The authors then examined relative changes in imaging use between the two groups over different periods of time.
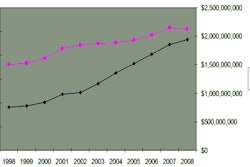
They found that advanced imaging use in the group with stage IV cancer increased by 4.6% from 1995 to 2006, while it declined 2.5% in the group with stage I and II cancer. Also, while the average number of scans per-person per-month increased among those with earlier-stage disease, it did so at a lower rate than in those with stage IV cancer.
The authors also examined the use of imaging by time period, from a "diagnostic" phase at the beginning of patient management through a "continuing-care" phase to an "end-of-life" phase. The diagnostic phase was the only phase in which the use of imaging grew more rapidly among early-stage patients than stage IV patients; after this phase, the rates of imaging for early-stage patients either declined or grew less rapidly than for stage IV patients.
More therapy options?
In discussing the results, the authors noted that the expansion in imaging for stage IV patients is most likely due to the increasing number and types of treatment available, as imaging is often used to monitor treatment and disease progression. That said, even though cancer treatments have been changing, survival for patients with stage IV disease has only changed modestly, they wrote.
The authors also noted that there are few guidelines covering the use of imaging in patients with advanced disease -- the group that saw the most growth in imaging utilization. On the other hand, during the study period, a number of national guidelines were published calling for more limited use of imaging for surveillance of patients with stage I and II disease, and it was in this group that imaging use declined outside of the initial diagnostic period.
For patients with advanced disease, quality of life should be among the primary outcomes assessed, according to the authors, and routine use of imaging could distract patients and caregivers from this goal.
The call to develop more comprehensive guidelines for imaging use in stage IV patients was echoed in an accompanying editorial by epidemiologists K. Robin Yabroff, PhD, and Joan Warren, PhD, of the U.S. National Cancer Institute's Health Services and Economics Branch.
They recommend that such "guidelines must be informed by better evidence about the incremental benefit of advanced imaging over other technologies in guiding a multitude of clinical decisions, not only comparisons of the technical quality of images."
Yabroff and Warren endorsed the idea of analyzing imaging use by phases of time from diagnosis. They also believe that information contained in electronic medical records documenting the use of advanced imaging in these patients could help the development of guidelines that either do not exist or are minimally available.