When it comes to the reliability of radiologic reads, there is no substitute for experience, especially among second-year radiology residents and first-year staff physicians.
A new study from the University of Iowa Carver College of Medicine in Iowa City found that the error rate for radiograph interpretations will decrease with experience and, predictably, first-year residents have the highest rate of missed diagnoses. One interesting note from the study, however, is that first-year board-certified radiologists had a major error rate similar to that of experienced board-certified radiologists.
In presenting research results at the 2008 American Roentgen Ray Society (ARRS) annual meeting in Washington, DC, Dr. D. Lee Bennett, associate professor of radiology at the Carver College of Medicine, said the study is important because many medical centers rely on residents to provide preliminary readings during off-hours without immediate assistance from more experienced, in-house staff physicians. First-year staff physicians also interpret and report radiology images without oversight from an experienced attending physician during all hours at practices throughout the U.S.
Because residents and first-year staff physicians are less experienced, Bennett said, they are prone to errors, which is a concern for emergency physicians who rely on accurate interpretations to care for critically ill patients.
Previous research
In his ARRS presentation, Bennett cited previous studies that have shown error rates between 3.5% and 4% among radiologists in practices (American Journal of Roentgenology, September 2007, Vol. 189:3, pp. 517-522). One other study concluded the major error rate of radiographs is between 1% and 1.5% for early trainees and between 0.3% and 0.5% for more experienced radiologists (Emergency Radiology, February 2007, Vol. 13:5, pp. 231-235).
The University of Iowa retrospective study reviewed emergency room radiographs from July 2006 through December 2006, calculating and accounting for missed interpretations and major errors by residents, first-year staff physicians, and physicians with experience of two years or more. All radiographs and medical records were evaluated by two radiologists and one medical student.
The study defined a major error as one that "resulted in a change of treatment, increased morbidity, a need for additional imaging, or considered an emergent or unexpected significant finding that should be directly communicated to the referring physician."
Study results
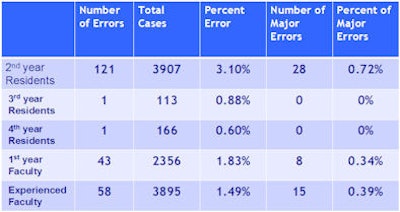
Researchers found that residents had 123 discrepancies (2.9%) among a total of 4,186 cases, while first-year faculty had 43 discrepancies (1.8%) among 2,356 cases. Attending physicians were responsible for 58 discrepancies (1.5%) among 3,895 cases.

When the results are segmented among residents, first-year residents had no discrepancies in 82 cases, second-year residents had 121 (3.1%) discrepancies in 3,907 cases, and there was one (0.9%) discrepancy in 113 cases for third-year residents. Fourth-year residents had one (0.6%) discrepancy in 166 cases.
All residents had a total of 28 (0.7%) major errors, while first-year faculty recorded eight (0.3%) major errors and attending physicians had 15 (0.4%).
In a comparison with previous research, Bennett noted that in the Iowa study, the error rate decreased from 1.6% to 0.7% among radiology residents who had their start-of-call delayed to their second year of residency. However, second-year residents who had started their calls in the first year of residency had fewer errors than second-year residents with no previous call experience.
"Part of that learning process is when you are on your own ... and developing self-confidence," Bennett said. "We found out that there was a statistically significant decrease in the major error rate by residents if they waited until July 1 of their second year to start [taking calls]. However, they were not as good as second-year residents who started taking calls in their first year."
Major errors
Of the 51 major errors, pneumonia was the most common omission (18 cases), followed by vertebral fractures (12 missed cases) and clavicle fractures (seven missed cases). All other injuries had frequencies of less than three.
Bennett said the missed diagnoses are common errors among all radiologists but are more frequent among less experienced readers. "Those are the same types of errors that people tend to miss when they are in practice," he added, "but they don't miss it as often as the younger people did."
The study also looked at first-year faculty who had finished their residencies, had become board-certified radiologists, and were making calls on their own. The overall error rate was higher in this category. Bennett opined that the increase may be the result of false-positive rates. A radiologist who puts his or her name to the report may not want to be responsible for missing something significant.
Bennett and his colleagues plan to continue their research in regard to false-positive rates and "overcalling" some diagnoses. "One thing I'd really like to look at is to see if the false-positive rate is higher in someone with experience and what is leading to those errors," he said.
By Wayne Forrest
AuntMinnie.com staff writer
May 28, 2008
Related Reading
Residents' on-call CT reads comparable to faculty's final reports, January 1, 2008
Residents' reads reliable, study says, September 19, 2007
Revisiting report errors serves as educational tool for residents, December 22, 2005
Most rad residents OK with on-call preparation, duty, November 14, 2005
Copyright © 2008 AuntMinnie.com