CHICAGO - Spiral CT may be too fast for its own good -- at least for radiotherapy treatment planning of the thorax. A presenter at RSNA’s radiation oncology scientific sessions Monday said that spiral CT, particularly in 3-D conformal radiation therapy, may not represent the time-averaged location of thoracic tumors because it’s faster than heart and lung cycles. For these applications, axial CT’s slower pace may win the race.
Dr. Katherine Mah from the Toronto-Sunnybrook Regional Cancer Center presented a study designed to investigate the hypothesis that the standard mode for CT simulation, spiral scanning, may not accurately yield the time-averaged position of thoracic tumors during radiation therapy.
“CT-based treatment planning assumes that the static images taken during free breathing represent the time-averaged position of the tumor during the few minutes that it takes to deliver the treatment,” Mah said. “In the 1980s, the conventional CT planning was based on axial mode acquisitions, typically taking 3-4 seconds per image, giving you a time-averaged position representative of one breathing cycle and many cardiac cycles. However, 3-D CT simulation relies exclusively on the use of spiral CT technology, in which data for each image are acquired in generally less than one second.”
However, without the use of breathhold or gating techniques, the faster spiral CT mode can potentially create a new problem, Mah said.
“If the spiral-defined tumor does not represent the time-averaged position of the tumor during treatment, then significant underdosing may occur, particularly in 3-D conformal radiation therapy, where tight and generally symmetric margins are placed around the identified tumor to account for internal motion.”
Doctors at the Canadian center began to suspect this was precisely the problem after they found a geometric discordance of 5 mm or more at well-defined tumor boundaries in four of 20 patients – despite careful co-registration between FDG-PET hybrid and CT simulations designed to eliminate external setup variations.
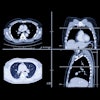
To investigate the hypothesis, a patient with a well-defined parenchymal lesion in the left upper lobe underwent spiral CT followed immediately followed by a 4-second axial mode scan. In addition, the location of the tumor fairly far out on the chest wall would tend to minimize the motion effect, Mah said.
For both types of scans, the researchers used a PQ5000 CT (Marconi Medical Systems, Cleveland) scanner with 3-mm slice thickness and spacing, a 48-cm field of view, 130 kV, 200 mAs per rotation with a pitch of 1.5. Only the acquisition time, 0.7 seconds for spiral CT vs. 4 seconds for axial, was different.
The resulting datasets were objectively localized using an autocontouring tool, and the countours were plotted together. The volume based on the spiral scan was about 55 cc, while the volume outlined on the axial mode was about 61 cc, an increase of approximately 11%.
The differences weren’t limited to volume; the researchers also noted an anterior shift.
“In this slice, you can see that the spiral-based contour has also been shifted by approximately 7 to 8 mm,” Mah said. “If you look at the volume overlap, this volume is about 70% relative to the total axial volume. And this is out of a maximum possible overlap volume of 89%, taking into account the differences in the total volume between the two modalities.”
Plotting the differences in the centers of the mass between the modalities confirmed a 5-mm anterior shift, leading the researchers to postulate a third cause beyond breathing and heart motion.
“We speculate that this may represent patient relaxation between the spiral mode and the axial mode, a phenomenon that has been recorded in the literature, and seen in setting up patients between simulation and subsequent treatment,” Mah said.
“In conclusion, I’d like to say that spiral CT may not represent the time-averaged location of the thoracic tumor. For 3-D [conformal radiation therapy], these findings emphasize the need for adequate margins to account for the full range of internal motion, acknowledging that the spiral CT may capture an extreme position -- the extent of this problem being greatest for small lesions, and for lesions located closest to the diaphragm.”
The next phase of the study would study tumors in different areas of the chest, and also coordinate the results with FDG-hybrid PET imaging, Mah said.
By Eric Barnes
AuntMinnie.com staff writer
November 28, 2000
Dr. Katherine Mah from the Toronto-Sunnybrook Regional Cancer Center presented a study designed to investigate the hypothesis that the standard mode for CT simulation, spiral scanning, may not accurately yield the time-averaged position of thoracic tumors during radiation therapy.
“CT-based treatment planning assumes that the static images taken during free breathing represent the time-averaged position of the tumor during the few minutes that it takes to deliver the treatment,” Mah said. “In the 1980s, the conventional CT planning was based on axial mode acquisitions, typically taking 3-4 seconds per image, giving you a time-averaged position representative of one breathing cycle and many cardiac cycles. However, 3-D CT simulation relies exclusively on the use of spiral CT technology, in which data for each image are acquired in generally less than one second.”
However, without the use of breathhold or gating techniques, the faster spiral CT mode can potentially create a new problem, Mah said.
“If the spiral-defined tumor does not represent the time-averaged position of the tumor during treatment, then significant underdosing may occur, particularly in 3-D conformal radiation therapy, where tight and generally symmetric margins are placed around the identified tumor to account for internal motion.”
Doctors at the Canadian center began to suspect this was precisely the problem after they found a geometric discordance of 5 mm or more at well-defined tumor boundaries in four of 20 patients – despite careful co-registration between FDG-PET hybrid and CT simulations designed to eliminate external setup variations.
To investigate the hypothesis, a patient with a well-defined parenchymal lesion in the left upper lobe underwent spiral CT followed immediately followed by a 4-second axial mode scan. In addition, the location of the tumor fairly far out on the chest wall would tend to minimize the motion effect, Mah said.
For both types of scans, the researchers used a PQ5000 CT (Marconi Medical Systems, Cleveland) scanner with 3-mm slice thickness and spacing, a 48-cm field of view, 130 kV, 200 mAs per rotation with a pitch of 1.5. Only the acquisition time, 0.7 seconds for spiral CT vs. 4 seconds for axial, was different.
The resulting datasets were objectively localized using an autocontouring tool, and the countours were plotted together. The volume based on the spiral scan was about 55 cc, while the volume outlined on the axial mode was about 61 cc, an increase of approximately 11%.
The differences weren’t limited to volume; the researchers also noted an anterior shift.
“In this slice, you can see that the spiral-based contour has also been shifted by approximately 7 to 8 mm,” Mah said. “If you look at the volume overlap, this volume is about 70% relative to the total axial volume. And this is out of a maximum possible overlap volume of 89%, taking into account the differences in the total volume between the two modalities.”
Plotting the differences in the centers of the mass between the modalities confirmed a 5-mm anterior shift, leading the researchers to postulate a third cause beyond breathing and heart motion.
“We speculate that this may represent patient relaxation between the spiral mode and the axial mode, a phenomenon that has been recorded in the literature, and seen in setting up patients between simulation and subsequent treatment,” Mah said.
“In conclusion, I’d like to say that spiral CT may not represent the time-averaged location of the thoracic tumor. For 3-D [conformal radiation therapy], these findings emphasize the need for adequate margins to account for the full range of internal motion, acknowledging that the spiral CT may capture an extreme position -- the extent of this problem being greatest for small lesions, and for lesions located closest to the diaphragm.”
The next phase of the study would study tumors in different areas of the chest, and also coordinate the results with FDG-hybrid PET imaging, Mah said.
By Eric Barnes
AuntMinnie.com staff writer
November 28, 2000
Copyright © 2000 AuntMinnie.com
Click here to view the rest of AuntMinnie’s coverage of the 2000 RSNA conference.
Click here to post your comments about this story.