Recent studies have shown virtual colonoscopy to have a high sensitivity -- 75% to 100% -- for detecting the colorectal polyps sized 10 mm and larger that are considered clinically significant.
The research has been criticized, however, for its reliance on high-risk cohorts, including patients who have a history of polyps or cancer, or who present with blood in the stool or other symptoms that are suggestive of colorectal cancer.
Virtual colonoscopy being an exclusively diagnostic exam (rather than diagnostic and therapeutic like conventional colonoscopy), patients whose polyps are detected in VC must proceed to conventional colonoscopy to have them removed. On the other hand, it is presumed that low-risk patients will generate mostly negative virtual colonoscopy results, obviating the need for a second procedure, and making widespread VC screening feasible.
Studies of lower-risk patients have been few and far between. But at the 2002 RSNA meeting in Chicago, Dr. Michael Macari from New York University Medical Center in New York City discussed one of the first studies to evaluate virtual colonoscopy results in a screening population.
"The question is, will CT colonography perform as well in a screening population where the prevalence of disease is lower, and perhaps 5 in 100 patients will have a 10-mm colorectal polyp? Large datasets need to be evaluated, especially with multidetector-row (CT) in order to detect these relatively few polyps," he said.
Part of the problem is that biases can potentially arise when examining so-called "polyp-rich" patient cohorts, Macari added.
"If you think a polyp is present, you're going to look at the (CT) data until you find it," he said. "Indeed, if you look at the results of many of these papers, you'll find interpretation times of 30 minutes or even more. And clearly that is not a clinically feasible amount of time when we're talking about radiologists in the community performing CT screening."
In the ongoing study, the group has prospectively evaluated 68 asymptomatic male patients (mean age 60) with both virtual colonoscopy and conventional colonoscopy, using the latter as a reference standard. Macari and colleagues found that VC produced excellent results with clinically significant polyps, but detected smaller lesions less successfully.
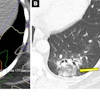
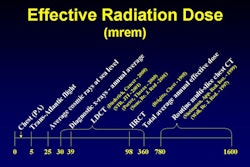
All of the subjects underwent bowel preparation as recommended by the gastroenterologist, followed by colonic insufflation with room air, then virtual colonoscopy and same-day conventional colonoscopy. Prone and supine images were acquired on a 4-row multidetector-row Somatom Volume Zoom scanner (Siemens Medical Solutions USA, Malvern, PA) using a low-dose protocol consisting of 120 kVp, 50 mAs, 4 x 1-mm collimation, and 1.25-mm effective slice width.
The group evaluated axial CT data using a cine method to reduce interpretation time. Multiplanar reconstructions (MPR) and 3-D views were added as needed for problem solving. Virtual colonoscopy was performed by an experienced radiologist; colonoscopy by a board-certified gastroenterologist. Every biopsied lesion was sent for histological analysis, Macari said.
The conventional colonoscopy results were normal in 29/68 (43%) of patients, while virtual colonoscopy produced normal results in 26/68 (38%) of patients; the three polyps not seen in conventional colonoscopy were considered false-positive results.
In the remaining 39 patients, conventional colonoscopy detected a total of 91 colorectal polyps, only 22 (24%) of which were visible in virtual colonoscopy, Macari said.
"But when we look at the results, and we break down the colorectal lesion in terms of size, the vast majority of lesions that we missed were 5 mm or smaller," he said. Virtual colonoscopy detected just 14% of lesions 5 mm and smaller, 56% of lesions 5-9 mm, and 100% (n=3) of lesions 10 mm and larger.
Three of the 7 lesions measuring 6-9 mm were hyperplastic polyps or normal colonic mucosal protrusions; excluding them raised the sensitivity from 69% to 75% in this category.
Virtual colonoscopy was found to have excellent sensitivity for polyps 10 mm and larger, and excellent specificity. The 9-minute average interpretation time (excluding dictation) was clinically reasonable, Macari said. And while the sensitivity for smaller lesions was clearly diminished, the benefit of reporting and following them remains controversial.
"If you see these diminutive lesions in virtual colonoscopy, what do you do with them?" he said. "Do you subject the patient to a colonoscopy for an 8-mm lesion that ultimately turns out to be a hyperplastic polyp...? Another important question is, what is the clinical or imaging follow-up for a patient who comes for a virtual colonoscopy and has a normal finding, when you know there are lesions that are missed?"
By Eric BarnesAuntMinnie.com staff writer
January 7, 2003
Related Reading
Low-dose CT colonography accurately detects large colorectal neoplasms, July 30, 2002
Virtual colonoscopy aces first flat-lesion study, December 3, 2002
VC screening trials find good sensitivity, high patient acceptance, October 30, 2002
In virtual colonoscopy, nothing beats a good prep, July 16, 2002
Copyright © 2003 AuntMinnie.com