The escalating use of CT for children who present in emergency departments is of well-documented concern. But a pair of new studies published in the November issue of Pediatric Radiology indicates that while the problem is serious, pediatric imaging advocates are making progress in addressing the issue.
CT radiation dose has risen rapidly for a variety of reasons, ranging from increasingly powerful CT technology to the growth of "defensive medicine" on the part of clinicians worried about malpractice litigation. Nowhere is this more evident than in the emergency department, where in the haste to reach a rapid diagnosis many children are being exposed to more radiation than necessary.
A special supplement to the November issue of Pediatric Radiology deals with the topic in detail (Pediatric Radiology, Vol. 38, Suppl. 4, pp. 625-734), offering articles on topics originally presented at the Society for Pediatric Radiology's February 2008 ALARA (As Low As Reasonably Achievable) meeting.
In one paper, Dr. Joshua Broder of Duke University Medical Center in Durham, NC, discusses the forces driving CT overutilization and presents possible solutions to the dilemma. In a second paper, Dr. Nathan Kuppermann of the University of California, Davis (UCD) Medical Center discusses whether CT scans are appropriate for children admitted to emergency departments with minor blunt head trauma.
Escalating utilization
Broder's paper traces the rise of pediatric CT use in the ED, based on experiences at Duke, where he is a surgeon and emergency medicine physician. While comprehensive statistics of CT scan utilization for pediatric patients admitted to emergency departments in the U.S. aren't available, Duke has seen CT utilization outpace emergency department volume growth by 15- to 200-fold between 2000 and 2006.
"During this time frame, the pediatric emergency department population increased by only 2%, with little change in the severity of illness assessed by triage acuity scores," Broder said. Triage acuity scores are validated measures of the need for immediate patient assessment and treatment, correlated to the likelihood of admission or ICU stay.
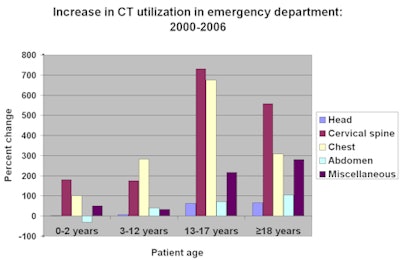
With the exception of abdominal CT scans of infants and children under two years of age, and head CT scans of children under the age of 12, the number of CT exams performed over a six-year span starting in 2000 increased between 34% and 731% for children ages 17 and under depending upon the type of examination, according to Broder. Usage for patients ages 18 and over increased between 66% and 557%.
 |
| Joshua Broder et al, Duke University Medical Center |
Growth in CT utilization was greatest among adolescents, Broder reported. He attributed this to the fact that because children appear more adult-like, physicians adopt diagnostic strategies used in the evaluation of adult patients. These include pan-CT (head, cervical spine, chest, abdomen, pelvis) for trauma evaluation, immediate use of CT for evaluation of abdominal pain, and CT scanning prior to specialty consultation rather than at the request of the specialist.
Overcrowded emergency departments
Because emergency departments are seriously overcrowded -- due in part to the reduction in the number of hospital emergency departments (by 370 between 1994 and 1999) -- and because of concern about litigation, emergency physicians are under enormous pressure to make a rapid diagnosis, according to Broder.
Broder proposes a number of solutions to reducing overutilization:
- Initiatives to educate physicians to the risks of pediatric radiation dose, such as the Image Gently campaign launched in January 2008
- Increased use of clinical decision rules to limit imaging use in cases where it most likely isn't required
- The incorporation of clinical decision rules into computerized physician order entry software, to require ED physicians to consider radiation risk before ordering tests
- The use of observation rather than immediate imaging in some cases
- Continued work on dose-reduction strategies for lower mA and kV settings on CT studies
- The use of nonionizing imaging modalities in the ED, such as by making ultrasound more widely available on an after-hours basis.
When to use CT for pediatric head trauma
Kuppermann's paper addressed the controversy of whether CT scans should be ordered for children admitted to emergency departments with minor blunt head trauma. Kuppermann, a pediatric emergency physician, also advocates the development and utilization of decision rules to reduce some of the more than 350,000 head CT scans ordered annually for these patients.
More than 650,000 children are admitted to emergency departments each year with symptoms of head trauma. Of these, approximately half have seemingly minor head trauma of documented traumatic brain injury.
Approximately 50% of the children admitted now receive head CT examinations, according to Kuppermann. Multiple studies have revealed that the prevalence of brain injury shown on CT is 5% or less, and surgical intervention is required in less than 1% with children who have an assessment of minor blunt head trauma and a Glasgow Coma Scale (GCS) score of 15 or higher.
The GCS score is considered an important predictor of a patient's mental status. A number of published clinical studies suggest that the risk of brain injury visible on CT in patients evaluated in an emergency department after blunt head trauma is 2%-3% with a GCS score of 15, 7%-8% with a GCS score of 14, and approximately 25% with a GCS score of 13.
Reliable and valid decision rules could play an important role in determining the need for CT head examinations for patients with a GCS score of 14 and 15, Kuppermann suggests. It is necessary for the rules to meet two criteria: be highly accurate and supported by evidence, and be simple enough to apply in practice.
The National Emergency X-Radiography Utilization Study II (NEXUS II) is an ongoing, prospective, multicenter study of blunt head trauma victims that was designed to derive and subsequently validate a decision aid to identify a group of head trauma patients who are at very low risk for significant intracranial injury, thus enabling a reduction in unwarranted cranial CT imaging. Kuppermann reported that a subanalysis study of 1,666 pediatric patients enrolled revealed that use of a single decision rule could have reduced the number of CT scans performed by 14%.
In a study of children presenting with head trauma to UCD Medical Center's emergency department between July 1998 and September 2001, researchers reported that of 1,271 children who had head CT scans performed (representing 62.2% of the total number of patients enrolled), traumatic brain injury was identified on CT for only 98 patients, or 7.7%. Had isolated loss of consciousness and/or amnesia been eliminated as an indication for cranial CT, the number of CT scans would have been reduced by 12%.
A multi-institutional prospective study enrolling 34,000 patients between June 2004 and September 2006 was conducted by the Pediatric Emergency Care Applied Research Network, headquartered at the Intermountain Injury Control Research Center in Salt Lake City. Findings are starting to be reported, and its objective is to identify high- and low-risk indicators of traumatic brain injury to create highly accurate and reliable prediction rules, including when CT head examinations are appropriate. The Pediatric Emergency Research of Canada network, headquartered in Calgary, Alberta, also is completing a similar prospective study, Kuppermann said.
"These two studies should provide the foundation of evidence not only to guide CT decisions by clinicians, but also to help parents participate in the decision-making process," he noted.
By Cynthia Keen
AuntMinnie.com staff writer
October 17, 2008
Related Reading
Cincinnati meeting starts long road to harmonizing CT dose displays, September 17, 2008
Study: Radiologists dial back on pediatric CT settings, September 4, 2008
Meeting to examine pediatric CT dose, August 18, 2008
CT experts grapple with rising concerns about radiation dose, May 14, 2008
Groups advocate less radiation for kids, January 23, 2008
Copyright © 2008 AuntMinnie.com


















