Virtual colonoscopy is technically feasible and less invasive than conventional colonoscopy for surveillance after sigmoid colostomy, according to a study in the October American Journal of Roentgenology. But better techniques are needed before it can be used routinely, the researchers said.
The exams were performed without problems except for one patient who had air and fluid leakage, wrote Dr. Ju Hee Lee, Dr. Seong Ho Park, and colleagues from Asan Medical Center in Seoul, Korea.
"Our findings suggest that [VC, also known as CT colonography or CTC] may be an option for colonic evaluation in patients who have undergone colostomy," they wrote. "Our results also revealed that CTC examinations in patients who have undergone colostomy have several unique technical aspects" (AJR, October 2011, Vol. 197:4, pp. W653-W657).
Those aspects include inadequate distention of the colon, which occurred more frequently in colostomy patients than in others undergoing screening CTC, a likely effect of maintaining lower intracolonic pressure than normal to avoid expulsion of the balloon catheter during the examination, according to Lee and his team. In addition, prone imaging isn't feasible postcolostomy, although decubitus-position imaging is a fair replacement.
CTC has advantages in surveillance of cancer patients because both postcolostomy colonic and extracolonic surveillance "are necessary because tumors can recur in both locations, more frequently in extracolonic organs than in the colon," wrote Lee and colleagues. Colonoscopy is limited to examining the colon. CTC with IV contrast media "inherently allows simultaneous examination of both the large intestine and extracolonic abdominal organs and may be a viable standalone technique for dual colonic-extracolonic surveillance after colorectal cancer surgery," they wrote.
In their study, Lee and colleagues aimed to evaluate "the technical feasibility of CTC of patients who have undergone sigmoid colostomy after abdominoperineal resection for rectal cancer," they explained.
The authors examined 18 patients (7 men, 11 women; mean age, 57.2 ± 14.5 years) who had undergone abdominoperineal resection with sigmoid colostomy for rectal cancer. They performed colonic cleansing with magnesium citrate and tagging with 5% weight-to-volume barium following a low-residue diet.
 |
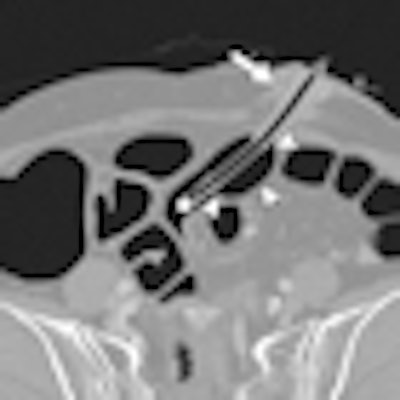
| Woman, 72, who had a sigmoid colostomy undergoes CTC. Oblique transverse CTC image shows position of catheter. Distended balloon (arrowheads) is located several centimeters beneath colostomy stoma. Short colonic segment and adjacent tissue between balloon and stoma (arrow) are squeezed as distended balloon is slightly pushed back during colonic insufflation, acting as mechanism to prevent expulsion of balloon catheter. Image republished with permission of the American Roentgen Ray Society, from AJR, October 2011, Vol. 197:4, pp. W653-W657. |
After cleansing, a standard small rectal catheter with a retention balloon (ProtoCO2l administration set, Bracco Diagnostics) was introduced into the colonic stoma. Unenhanced right-decubitus and contrast-enhanced 150-mL iopromide (Ultravist 300, Bayer HealthCare Pharmaceuticals) supine images were acquired at CTC (Somatom Sensation 16, Siemens Healthcare). A slice thickness of 0.75 mm, 120 kVp, and 50 mAs were used for the unenhanced acquisition, with an automated dose reduction set to a maximum of 200 mAs for the contrast-enhanced scan.
An inflated balloon was placed several centimeters below the skin for insufflation of the colon using automated CO2 distention, and "the interposed tissue acted as the mechanism for preventing balloon expulsion during colonic insufflation with carbon dioxide," the authors explained. Finally, the group documented air-fluid leaks, balloon expulsion, or complications, evaluating colonic distention on a four-point scale (4 = optimal).
A highly experienced reader examined the CTC images using a commercial CTC system (Xelis Colon, Infinitt Healthcare). Depending on CTC findings, patients were offered immediate conventional colonoscopy or routine colonic surveillance, and the researchers compared CTC and colonoscopy results when available.
"None of the 18 patients needed termination of a CTC examination because of technical failure or procedure-related complications, and no patient experienced expulsion of the ballooned catheter," Lee and colleagues reported. Mild air and fluid leakage was seen temporarily in one patient but resolved spontaneously. The mean amount of CO2 used was 2.64 ± 0.64 L.
CTC findings were normal in all 18 patients, as were colonoscopy results in all 10 patients who underwent colonoscopy a median 13 months after CTC.
Colonic distention graded on a scale of 1 to 4, with 4 being optimal
|
Four patients (22.2%) had segments that weren't adequately visualized in either position due to luminal collapse -- all involving the sigmoid colon. Three patients (16.7%) had areas submerged under fecal matter in both positions. Nevertheless, fecal tagging (n = 3) or IV contrast enhancement (n = 1) rendered these segments evaluable.
"CTC through a sigmoid colonic stoma is feasible with currently available instruments," Lee and colleagues wrote. "Our findings suggest that CTC may be an option for colonic evaluation in patients who have undergone colostomy." Still, several unique technical considerations apply to CTC in this population, they said.
Inadequate distention of the sigmoid colon was more frequent in the unique study population, probably related to efforts to maintain a lower intracolonic pressure than used for typical CTC. The lower pressure was chosen to avoid expulsion of the balloon catheter.
"We found that trapping of a short colonic segment and adjacent tissue between the balloon and the stoma, preventing expulsion of the catheter, worked effectively at the low intracolonic pressure used in our study, as evidenced by the nonoccurrence of catheter displacement or major leakage of air or fluid during the examinations," they wrote. "It is uncertain, however, whether the same method would work successfully at a higher colonic insufflation pressure."
Positioning
Use of the decubitus scan rather than the prone position increases the likelihood that some colonic surfaces and lesions will be submerged in all positions, the group wrote. This increases the need for adequate fecal tagging to overcome submergence of some surfaces and lesions, and contrast enhancement may also help depict untagged or poorly tagged residual matter.
As for limitations, the authors noted the small size of the study, the lack of conventional colonoscopy findings in all cases, and the lack of a formal patient evaluation process, though they said they were unaware of any patient complaints.
"Because CTC is generally better accepted by patients and is more convenient than colonoscopy, CTC is likely to be more acceptable to colostomy patients," Lee and colleagues wrote. "Moreover, dual colonic-extracolonic evaluation with CTC, an advantage in postsurgical surveillance of colorectal cancer patients, is not possible with colonoscopy."