An F-18 FDG-PET/CT scan proved crucial in identifying an ultrarare case of brain inflammation in a patient due to the flu, a team at Zibo Central Hospital in Zibo, China, has reported.
The patient was a 38-year-old woman who presented to the emergency department with a six-day fever, headache, and severe fatigue, and her brain and spinal cord MRI showed no abnormalities, reported nuclear medicine physician Hukui Sun, MD, and colleagues.
“Influenza B virus-associated encephalitis is rare, with an incidence of about 0.21 per million. Cerebellitis has never been described before to the best of our knowledge,” the group wrote. The case was published March 27 in the Journal of Nuclear Medicine.
The name cerebellum comes from Latin and means “little brain.” It is located at the back of the head, just above and behind where the spinal cord connects to the brain itself and plays a central role in maintaining gait, stance, balance, and coordinating complex movements.
In this case, the patient’s medical history was unremarkable, the authors explained. A blood serum tests confirmed influenza B virus and while her initial symptoms improved within 48 hours after antiviral treatment, neurologic manifestations (ataxia, dyskinesias, parkinsonism, and progressive dysuria) were gradually progressing, they noted.
Further, cerebrospinal fluid multiplex nucleic acid amplification tests were negative and a brain and spinal cord MRI showed no abnormalities.
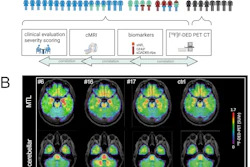
“However, F-18 FDG-PET/CT demonstrated extensive cerebellar cortex hypermetabolism. The SUVmax was 25.91,” the group wrote.
 Brain MRI and F-18 FDG brain and whole-body PET/CT images. (A) No obvious abnormalities were found in axial and sagittal slices from T2-weighted MR images. (B) Whole cerebellar cortex had diffuse F-18 FDG hypermetabolism in PET/CT brain images, with SUVmax of 25.91. (C and D) Whole-body F-18 FDG-PET/CT showing distended bladder. TLG = total lesion glycolysis; MTV = metabolic tumor volume. Image and caption courtesy of the Journal of Nuclear Medicine.
Brain MRI and F-18 FDG brain and whole-body PET/CT images. (A) No obvious abnormalities were found in axial and sagittal slices from T2-weighted MR images. (B) Whole cerebellar cortex had diffuse F-18 FDG hypermetabolism in PET/CT brain images, with SUVmax of 25.91. (C and D) Whole-body F-18 FDG-PET/CT showing distended bladder. TLG = total lesion glycolysis; MTV = metabolic tumor volume. Image and caption courtesy of the Journal of Nuclear Medicine.
The physicians immediately started the patient on intravenous acyclovir at a dose of 10 mg/kg every eight hours for 14 days and a five-day intravenous immunoglobulin cycle. In addition, she received intravenous methylprednisolone to reduce the inflammatory response in the central nervous system.
With continuous corticosteroid and physical therapy, her ataxia gradually improved, the group reported, and by the end of the second week, she was able to walk with only a slight limp and had improved coordination in her upper limbs.
Ultimately, the case highlights the importance of considering influenza B virus-associated neurologic complications in the cerebellum, the group wrote.
“PET/CT imaging was crucial as it provided information not shown by MRI, helping with the diagnosis and treatment guidance,” they concluded.
The full case report can be found here.













![A 53-year-old patient (patient number four) with a recurrent pituitary adenoma with extension of a cystic component of disease to the medial temporal lobe apparent on MRI (contoured in blue), and extension of disease to the left sphenoid bone and orbital apex apparent on [68Ga]Ga-DOTA-TATE (contoured in yellow).](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/04/pituitary-tumor.QGsEnyB4bU.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)



