By showing how four or more follow-up FDG-PET/CT scans for lung cancer can alter patient treatment plans, researchers at Johns Hopkins University are making the case for expanded Medicare reimbursement for these exams in a new article in the February edition of the Journal of Nuclear Medicine.
Currently, the U.S. Centers for Medicare and Medicaid Services (CMS) will pay for only three FDG-PET/CT scans when they are used to guide subsequent management of antitumor treatment after initial cancer therapy. Local Medicare administrative contractors must approve coverage for any additional FDG-PET/CT scans.
In light of that policy, the current study found that a fourth and subsequent FDG-PET/CT scans performed after primary treatment changed patient management in nearly one-third of the lung cancer exams reviewed (JNM, February 2015, Vol. 56:2, pp. 204-208).
The research "supports the suggestion that the number of follow-up scans performed for each patient should be planned on the basis of the individual-patient clinical context and cannot be generalized for the whole subset of lung cancer patients," wrote lead author Dr. Charles Marcus and colleagues.
FDG-PET/CT's record
FDG-PET/CT's effectiveness in oncology patients for staging, assessing therapy, and determining prognosis has long been established, and several studies have confirmed the hybrid modality's ability to change the treatment plan at the time of staging, the authors wrote.
However, there is "no substantial literature" exploring whether fourth and subsequent FDG-PET/CT exams can alter patient treatment plans, Marcus and colleagues noted. Therefore, they launched a retrospective study of patients at Johns Hopkins with biopsy-proven lung cancer who underwent more than three follow-up FDG-PET/CT scans after primary treatment between January 2001 and October 2013.
Eighty-five lung cancer patients (44 women and 41 men) met the inclusion criteria; the patients had undergone a total of 285 fourth and subsequent follow-up FDG-PET/CT scans (range, four to 28 scans per patient).
Sixty-one patients received four to six follow-up FDG-PET/CT scans, 17 had seven to 10 exams, and nine had more than 10 follow-up scans. A total of 112 scans were performed as the seventh or later follow-up exam.
The researchers tracked the patients until they died or until their last day of clinical follow-up. Median follow-up was 31.4 months (range, 0 to 155.2 months) from the fourth FDG-PET/CT scan.
Change in management
Of the 285 PET/CT scans, 149 (52%) were positive and 136 (48%) were negative for recurrence or metastasis, the researchers found.
The majority (219, or 77%) of the scans were conducted as routine follow-up without clinical suspicion of recurrent disease or metastasis. FDG-PET/CT identified recurrence or metastasis of lung cancer in 97 scans (44%) with no prior clinical suspicion, and it ruled out recurrence or metastasis in 16 scans (24%) conducted with prior clinical suspicion.
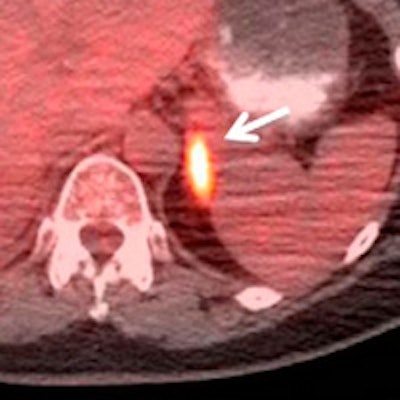
 Fused PET/CT images of a 60-year-old woman with stage IIB adenocarcinoma of the right upper lobe of the lung. A routine fifth follow-up scan was requested without prior clinical suspicion of lung cancer recurrence one year after completion of primary treatment. PET/CT shows hypermetabolic, metastatic multiple osseous (arrow) and left adrenal lesions (arrow). The patient was started on a new chemotherapy regimen after the study. Images courtesy of JNM.
Fused PET/CT images of a 60-year-old woman with stage IIB adenocarcinoma of the right upper lobe of the lung. A routine fifth follow-up scan was requested without prior clinical suspicion of lung cancer recurrence one year after completion of primary treatment. PET/CT shows hypermetabolic, metastatic multiple osseous (arrow) and left adrenal lesions (arrow). The patient was started on a new chemotherapy regimen after the study. Images courtesy of JNM.Among the 285 scans, 157 (55%) were performed on patients who were not being treated prior to FDG-PET/CT. Of those 157 scans, 99 (63%) resulted in no treatment changes, and the patients continued with their normal follow-up. The other 58 scans (37%) resulted in a change in treatment.
Of the 75 scans on patients who were treated prior to FDG-PET/CT, 53 (71%) prompted no treatment changes. However, treatment was altered based on 16 scans (21%), and treatment was stopped altogether after six other exams (8%). For 53 scans (19%), the effect on treatment was unknown.
Based on these findings, Marcus and colleagues concluded that a fourth and subsequent follow-up FDG-PET/CT studies changed the treatment strategy in nearly one-third (30%) of the patients.
"Though a behavior pattern of requesting routine follow-up scans is strongly discouraged, this study supports the suggestion that the number of follow-up scans performed for each patient should be planned on the basis of the individual-patient clinical context and cannot be generalized for the whole subset of lung cancer patients," they wrote.
The researchers noted several limitations of the study, such as its retrospective design and the fact that indeterminate scan results were included. Also, the perspective of the clinician ordering the study was unknown, thus the researchers may have underestimated the clinical suspicion of lung cancer prior to the FDG-PET/CT scans.


















