A new study from the University of Wisconsin School of Medicine and Public Health indicates that false-positive MRI diagnoses of medial meniscal tears are more common for longitudinal tears than for other tear types.
The researchers also concluded that false-positive MRI diagnoses are more common with MRI abnormalities at either the superior surface or the meniscocapsular junction.
Details are published in the July issue of the American Journal of Roentgenology (July 2008, Vol. 191:1, pp. 93-99). The authors, Dr. Arthur De Smet from the University of Wisconsin School of Medicine and Public Health in Madison and colleagues from other institutions, noted that spontaneous healing of longitudinal tears contributes to some of the false-positive MR diagnoses.
The researchers reviewed electronic medical records of 1,963 patients who underwent knee MRI examinations at the university from October 2001 through June 2004. The sample for the study was whittled to 559 patients based on certain criteria.
De Smet and colleagues chose patients who received an MRI exam on a 1.5-tesla magnet; their records included medical history and physical examination findings, there was no history of meniscal surgery, and patients had received knee arthroscopy after the MRI.
Patient parameters
From the final sample, researchers further defined clinical parameters to determine the patient's knee injury or atraumatic onset of knee pain, the time between the onset of knee symptoms and MR examination, and the time between the MR examination and knee arthroscopy. The criteria were chosen to calculate any healing effect related to the injury or the time it took for the healing to occur.
MRI exams were performed on a Signa 1.5-tesla magnet (GE Healthcare, Chalfont St. Giles, U.K.) with a four-channel knee phased-array coil and fast spin-echo imaging. The field-of-view was 14 cm, with a slice thickness of 3 mm with 1.5-mm interslice gap.
The retrospective review found 355 torn and 204 intact medial menisci through arthroscopy, with an original MR sensitivity for diagnosing medial meniscal tears of 97% (343 of 355 cases) and a specificity of 84% (172 of 204). The lowest positive predictive value (PPV) was 64% (32 of 50) for longitudinal tears and greatly lagged the PPV results for bucket-handle (25 of 25), complex (116 of 166), flap (60 of 66), and horizontal (84 of 87) tears.
The PPV for a longitudinal tear also was much lower than the value for radial (11 of 13) and root tears (15 of 18), but researchers concluded that the results in those situations were not significantly different.
 |
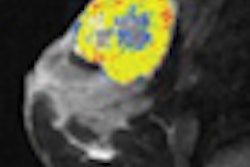
| Thirty-six-year-old man who had injured his knee while squatting down with true-positive MR diagnosis of medial meniscal tear at meniscocapsular junction on MRI 21 days after injury; tear was confirmed at arthroscopy 30 days after injury. Anterior cruciate ligament tear was not identified. Sagittal proton density-weighted (above) and T2-weighted (below) images show linear intermediate-signal-intensity line (arrow in above image) and intermediate- and less-than-fluid-intensity line (arrow in below image) contacting superior surface of meniscus. Fig. 2a, b. De Smet AA, Nathan DH, Graf BK, Haaland BA, Fine JP. Clinical and MRI findings associated with false-positive knee MR diagnoses of medial meniscal tears. AJR. 2008;191(1):93-99. Images courtesy of the American Journal of Roentgenology and the American Roentgen Ray Society. |
 |
PPV factor
In addition, the analysis found the PPV for medial meniscal tears was significantly higher at 97% (141 of 146) in patients with spontaneous onset of knee pain, compared with 88% (202 of 229) for patients with a specific knee injury. The PPV for medial meniscal tears also was significantly higher at 96% (270 of 282) for patients without an anterior cruciate ligament (ACL) tear, compared with 78% (73 of 93) for those with an ACL tear.
The study also confirmed that the majority of false-positive MRI diagnoses of medial meniscal tears are apparent longitudinal tears in the posterior horn.
Eighteen of 32 false-positive diagnoses occurred in those tears. In addition, MRI diagnosis of a longitudinal tear displayed a significantly lower PPV than complex, bucket-handle, flap, or horizontal tears and a lower value than a radial or root tear. The researchers concluded that the lack of significant difference between longitudinal, radial, and root tears "may reflect the small number of root and radial tears in our study group."
In other comparisons, the study found no significant difference in PPV for tears in different locations. With 285 of the 375 tears diagnosed on MRI in the posterior horn, the team noted that significant differences might not have been detected at locations with a lower frequency of tear. The study did find that the PPV decreased when patients had an acute knee injury rather than chronic pain and when patients had an ACL tear.
In their analysis, the authors wrote that despite the "initial hypothesis that spontaneous tear healing would increase with the delay between the initial injury and surgery, we found that PPV was not lower with longer MRI or operative delay. We had expected that with longer delays, a tear would be more likely to heal spontaneously."
Eight-nine percent of the patients with false-positive diagnoses had an interval of more than six weeks from injury to arthroscopy, the report also noted. "Apparently, this six-week interval is sufficient for healing to occur, so an increasing time for healing is not an important factor in determining the potential for spontaneous healing," the authors wrote.
Study limitations
The authors cited several potential limitations, including the division of peripheral tears on MRI into meniscocapsular junction compared to the outer one-third. "Our surgeons performing arthroscopy seldom use the term 'meniscocapsular separation,' because distinguishing a partial or a healed meniscocapsular junction injury from a deep sulcus can be difficult," the report noted.
T2-weighted images were used to make the distinction. "The retrospective reviewer," the authors continued, "found this distinction occasionally difficult, because edema related to the injury resulted in the posterior margin of the meniscus not always being clearly defined."
Another limitation may have been the use of fast spin-echo imaging to diagnose meniscal tears. While one previous study (AJR, July 2005, Vol. 184:1, pp. 1740-1743) found that fast spin-echo imaging has a lower sensitivity for meniscal tears, more recent research (AJR, October 2006, Vol. 187:4, pp. 911-914) discovered no significant change in sensitivity or specificity with fast spin-echo imaging compared with conventional spin-echo imaging.
The authors also cautioned as a possible limitation their decision to consider original MRI diagnoses of a possible tear based on the presence of a meniscal abnormality on only one image as a tear. The choice was made because "most published studies on MR accuracy for the diagnosis of a meniscal tear consider MRI findings to be positive for a tear if one or more images show abnormal findings," according to the authors. "If we had considered these MR diagnoses of a possible tear as not torn, we would have had fewer false-positive MR studies."
By Wayne Forrest
AuntMinnie.com staff writer
July 8, 2008
Related Reading
CAD shows potential for knee MR studies, May 26, 2008
Musculoskeletal US gets high marks for cost-effectiveness, May 2, 2008
U.K. study finds direct access to knee MRI is cost-effective, April 3, 2008
Ultrasound performs well in meniscal tears, February 5, 2008
Comprehensive musculoskeletal US exam offers most value, January 3, 2008
Copyright © 2008 AuntMinnie.com