Considering a patient's symptoms as noted on a short pre-MR imaging questionnaire improves radiologists' lumbar spine exam interpretation and diagnosis, researchers have found.
A team led by study senior author William Palmer, MD, of Massachusetts General Hospital in Boston found that radiologists who had access to information on patients' symptoms when they interpreted MRI spine exams achieved "a near statistically perfect agreement with spine specialists." The results were published October 29 in Radiology.
"The questionnaire is important because it obtains symptom information directly from patients and communicates it to radiologists at the time of lumbar spine MRI interpretation," Palmer said in a statement released by the RSNA.
MR imaging is the go-to modality for patients with back pain or sciatica because it can visualize degenerative and structural abnormalities of the spine, Palmer and colleagues explained. But MRI can show spinal abnormalities in patients with no symptoms of disease, and because "the same abnormalities can occur in both symptomatic and asymptomatic individuals, it is impossible to distinguish an incidental MRI finding from the true cause of pain by only looking at the MRI," they wrote, noting that "dictated reports may become lists of findings that cannot be ranked in order of diagnostic importance."
That's why it's crucial to correlate irregularities found on spinal MRI with patient symptoms, according to the authors. Palmer's team explored whether symptom information collected by a questionnaire could improve diagnosis via a study that included 240 patients who completed one undergoing lumbar spine MR imaging between May 2022 and February 2023. Patients noted the severity of their pain, where it was located, and what made it worse or better. A group of musculoskeletal radiologists with two to 24 years of spinal MRI interpretation experience alternated reading the exams with or without symptom information from patient questionnaires. Their diagnoses were then compared to those of spine specialists using Cohen kappa values.
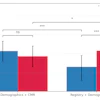
Palmer and colleagues found the following:
- Agreements on pain generators between radiologists and specialists were "almost perfect" for interpretations using symptom questionnaire results (kappa, 0.82 and 0.88 respectively, with 1 as reference).
- These agreements were "only fair to moderate for interpretations not using symptom questionnaire results (kappa, 0.26).
- Diagnostic certainty was higher for those MRI exam readings that included data from patients' symptom questionnaires compared with those that did not (mean, 80.4 vs. 60.5 [out of a scale of 0 to 100, with higher values indicating more certainty]).
- Interrater agreements were "substantial" when patient symptom information was used with MRI exam interpretation (kappa, 0.65) but only "fair to moderate" when it was not (kappa, 0.24).
"By distinguishing actionable pain generators from incidental findings, radiologists can best help primary care physicians who depend on MRI reports to guide their treatments and referrals," Palmer said.
In an accompanying commentary, Masis Isikbay, MD, and Vinil Shah, MD, both of the University of California, San Francisco, wrote that "the evaluation of lower back pain is a very common indication for advanced imaging, including MRI, but precise identification of the specific pain generator remains a challenging task."
"This is where an accurate and focused clinical history and examination can provide more clarity as to where the source of the pain may exist anatomically," Isikbay and Shah noted.
The complete study can be found here.