Doppler ultrasound-derived indices are not a reliable means of grading the severity of chronic liver disease, according to researchers from Hammersmith Hospital in London.
"None of the usually employed indices of portal hypertension (B-mode or Doppler) predicted ... cirrhosis in our group of patients with hepatitis-C chronic liver disease," said Dr. David Cosgrove during a presentation at the 2003 RSNA conference in Chicago.
While many authors have claimed that Doppler ultrasound indices are valuable for grading and assessing diffuse liver disease, the reproducibility and reliability of the techniques are controversial. A variety of techniques have been proposed, using B-mode (vessel caliber, caudate lobe hypertrophy) and Doppler (hepatic artery [HA] and portal vein [PV] velocities/ratios), Doppler perfusion index (DPI), and congestion index (CI).
To assess the indices, the Hammersmith researchers performed a prospective study on 65 patients with biopsy-proven hepatitis C virus (HCV)-related liver disease. Blinded to the histology results, a single experienced sonologist and radiologist performed ultrasound studies using a Sequoia scanner (Siemens Medical Solutions, Malvern, PA).
The average time from biopsy to ultrasound scan was 9.3 months. Vessel B-mode and Doppler measurements were taken, and the spleen and caudate lobe was assessed.
Measurements included:
- Caliber (maximum portal vein diameter and circumference).
- Peak velocity (main hepatic artery velocity, angle corrected; main portal vein velocity, angle corrected).
Ratios included:
- HA resistive index (peak systolic-end diastolic/peak systolic).
- Portal vein congestion index (portal vein area/portal vein velocity).
- Hepatic artery velocity (HAVmax) / portal vein velocity (PVVmax).
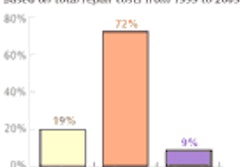
Of the 65 patients, 20 had mild hepatitis, 25 had moderate to severe hepatitis, and 20 had cirrhosis. The researchers encountered technical difficulties in the course of the study, and were able to obtain optimal hepatic arterial traces in only 30 patients, hepatic artery circumference in eight patients, and portal vein circumference in 18 patients, Cosgrove said. In addition, the Doppler perfusion index couldn’t be assessed.
The study team found no significant differences in the Doppler indices with increasing liver disease severity. An abnormal hepatic vein trace (i.e. biphasic or monophasic) was found in five of 17 patients (29%) with mild hepatitis, compared to 11 of 20 (55%) of patients with moderate/severe hepatitis, and 12 of 20 (60%) patients with cirrhosis.
Only spleen length correlated with stage and grade, but there was no clear separation between the categories, Cosgrove said. The group concluded that none of the often-utilized B-mode or Doppler indices for portal hypertension predicted cirrhosis in the study population.
"Perhaps this was because this disease behaves differently from alcoholic cirrhosis, for example," Cosgrove told AuntMinnie.com. He noted, however, that microbubble contrast tracer methods show promise in this application.
"The measurement of the time for a bolus of microbubbles to reach the hepatic veins (a measure of shunting in the liver) is easy to make with the new bubble-specific software and seems to be very reliable," he said.
By Erik L. RidleyAuntMinnie.com staff writer
February 26, 2004
Related Reading
Ultrasound of the pancreas: Cystic and non-focal pathology, February 13, 2004
US calculates splenic volume within ten minutes, January 19, 2004
Ultrasound and molecular tests useful in predicting renal allograft survival, July 10, 2003
Ultrasound effective in diagnosis, treatment of cystic liver lesions, May 15, 2003
Copyright © 2004 AuntMinnie.com