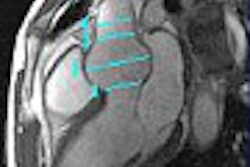
Renal sonography can effectively establish or exclude HIV-associated nephropathy (HIVAN), according to research published in the May issue of the Journal of Ultrasound in Medicine.
"This study reveals that patients with HIVAN have significantly increased renal echogenicity in comparison with HIV-infected patients with other renal diseases at the time of renal biopsy," wrote a multidisciplinary research team led by Dr. Mohamed Atta from Johns Hopkins University in Baltimore. "In addition, our study shows that the highest level of echogenicity based on a standardized measure is a strong predictor of HIVAN, and the lowest levels of renal echogenicity may be useful in excluding the diagnosis of HIVAN."
The team evaluated 87 HIV-positive patients who underwent both kidney biopsy and renal sonography after referral to the Johns Hopkins Renal Clinic from January 1995 to July 2002 JUM, May 2004, Vol. 23:5, pp. 603-610).
In 62 patients, sonographic images were clinically available. While specific probes were not identifiable for each sonographic image, commercially available broadband curved or vector transducers in the 2-to-5 MHz range are used in the institution's department of radiology, according to the researchers.
A radiologist performed an independent review of all available sonographic images. While aware that he was participating in a study of HIV patients, the radiologist was blinded to the clinical status, biopsy reports, and prior sonographic reports. To provide intra-rater reliability statistics, a second blinded review was performed on 39 sonographic images available from the first 29 patients.
The researchers graded renal echogenicity using a standardized score with four categories:
- 0 - The renal cortex was less echogenic than the liver.
- I - The renal cortex and liver were equally echogenic.
- II - The renal cortex was more echogenic than the liver.
- III - The renal cortex and renal sinus were equally echogenic.
Grading was performed for the right kidney only, and the echogenicity was presumed to be similar bilaterally.
The size of the kidney was also determined on each image, with a size of 12 cm or more defined as large. No liver abnormalities were noted on any of the sonographic readings. As none of the study participants were obese, body fat interference with the sonographic readings was considered insignificant.
Thirty-four patients (39%) had biopsy-proven HIVAN; the sensitivity and specificity for the two highest levels of echogenicity were 96% and 51%, respectively, with the highest level of echogenicity coming in at 40% and 95%, respectively.
The likelihood ratio for the diagnosis of HIVAN on the basis of the highest echogenicity score was 7.4 (95% confidence interval, 1.3-73.0; p=0.006), and 0.08 for the lowest two echogenicity scores (95% confidence interval, 0.002-0.57;p=0.003).
Kidney size was not associated with HIV-associated nephropathy status, the researchers noted.
"We have shown that sonographically based determination of renal echogenicity has diagnostic utility as a noninvasive procedure in the diagnosis of HIVAN in patients with echogenicity scores of 0, I, or III," the authors wrote. "As expected for acute nephropathy, patients with HIV disease and renal involvement do not have small or large kidneys. Thus, kidney size has no specific diagnostic utility in this group of patients."
By Erik L. Ridley
AuntMinnie.com staff writer
April 27, 2004
PET imaging of macrophages may detect early HIV encephalitis, April 7, 2004
HIV-infected women often have reduced bone density, March 25, 2004
Ongoing brain injury detected in HIV patients on therapy, February 12, 2004
PET detects lymph node activation during HIV infection, September 19, 2003
Decreased BMD in HIV-infected patients not related to antiretroviral therapy, August 28, 2003
Copyright © 2004 AuntMinnie.com