Breast radiologists can distinguish masses from nonmass lesions on ultrasound, according to research published December 9 in Radiology.
Radiologists achieved moderate to substantial interreader agreement for classifying these lesions, and with high concordance rates, wrote a team led by Hye Joung Eom, MD, from the University of Ulsan in Seoul, South Korea.
“A standardized set of descriptors would facilitate clear communication between radiologists and referring physicians and serve as a foundation for research,” Eom and colleagues wrote. “Moreover, accurate recognition of nonmass lesions is essential to ensure consistent diagnostic performance.”
Accurately recognizing nonmass lesions at breast ultrasound is needed for consistent diagnostic performance. Nonmass lesions on ultrasound often correspond to a developing asymmetry at mammography or nonmass enhancement at MRI.
However, there is overlap in features for both benign and malignant lesions. The latest edition of BI-RADS has nonmass lesions as a distinct category for breast radiologists to refer to.
The Eom team highlighted that few studies have evaluated interreader agreement in distinguishing between masses and nonmass lesions. The team studied this and identified clinical and imaging features that support confidence in classifying lesions as nonmass lesions.
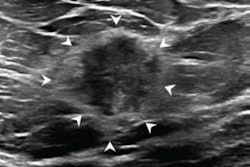
 Images depict a 50-year-old woman with a lesion detected during screening ultrasound. (A) Transverse and (B) longitudinal images reveal a 0.5-cm hypoechoic lesion (arrow) in the left breast. (C) Transverse color Doppler ultrasound image does not show an increase in vascularity. Two readers classified the lesion as a mass, whereas two others categorized it as a nonmass lesion, leading to its designation as a controversial nonmass lesion. Ultrasound-guided core needle biopsy and subsequent pathologic examination confirmed a nonproliferative breast change.RSNA
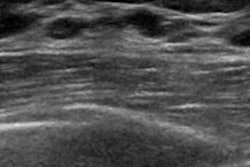
Images depict a 50-year-old woman with a lesion detected during screening ultrasound. (A) Transverse and (B) longitudinal images reveal a 0.5-cm hypoechoic lesion (arrow) in the left breast. (C) Transverse color Doppler ultrasound image does not show an increase in vascularity. Two readers classified the lesion as a mass, whereas two others categorized it as a nonmass lesion, leading to its designation as a controversial nonmass lesion. Ultrasound-guided core needle biopsy and subsequent pathologic examination confirmed a nonproliferative breast change.RSNA
Final analysis included 1,067 lesions in 912 women who underwent ultrasound-guided biopsy in 2021. Four breast radiologists participated in the study to assess interreader agreement in classifying lesions as either masses or nonmass lesions. An additional radiologist reclassified nonmass lesions that had conflicting interpretations. This radiologist labeled them as either definite or controversial nonmass lesions.
Of the total lesions, the additional radiologist classified 121 (11%) as definite nonmass lesions and 80 (7%) as controversial nonmass lesions.
The team reported the following findings:
The readers achieved moderate to substantial agreement (κ = 0.53 to 0.64), with a concordance rate of 84% to 91%.
The odds of being classified as a definite nonmass lesion were low for lesions smaller than 1 cm or having subtle architectural distortion (odds ratio [OR], 0.27; p = 0.003).
These odds were high for cases with echogenic foci associated with calcifications at mammography (OR, 2.68; p = 0.03) and microcysts (OR, 3.58; p = 0.02).
The presence of corresponding findings at mammography (p = 0.27) or MRI (p > 0.99) was comparable between the definite and controversial nonmass lesions.
The study authors wrote that small or subtle lesions can make it more challenging for radiologists to classify them as a mass or a nonmass lesion. They added that ultrasound findings of calcifications “appear to instill confidence in breast radiologists when they classify the lesion as a nonmass lesion.”
These findings support the widespread use of ultrasound for imaging nonmass lesions in clinical practice, wrote Regina Hooley, MD, from Yale University in New Haven, CT, in an accompanying editorial.
However, Hooley cautioned that designating a nonmass lesion as a breast ultrasound finding needs careful scanning and a complete diagnostic workup. She added that increased awareness and use of the nonmass lesion designation may lead to an increase in false-positive breast findings.
“Therefore, accurate and intentional use of nonmass lesions in the clinical setting is necessary to enhance the detection of early breast cancer and increase the sensitivity of breast ultrasound,” Hooley wrote. “Continued studies are needed to better understand the overall clinical utility and diagnostic accuracy of ultrasound nonmass lesions across multiple clinical settings.”
Read the full study here.