For years, magnetic resonance imaging has provided an invaluable window into problems of the musculoskeletal system, with the 1.5-tesla MRI scanner serving as the standard. But a new, higher standard is emerging that promises visible improvements in orthopedic imaging.
Three-tesla MRI scanners are now proliferating in clinical practice, as imaging groups choose to spend the extra $1 million or more that a new 3-tesla machine will cost compared to a current 1.5-tesla scanner.
Buying a 3-tesla scanner is an investment in increased signal-to-noise ratio, which enables either faster scanning or higher-resolution images than the 1.5-tesla norm. Patients are already benefiting from shorter exam times -- which can also reduce motion artifacts and the need for pediatric sedation -- and also from the increased diagnostic confidence that 3-tesla MRI brings to interpretation.
Musculoskeletal MR specialists are also looking forward to specific improvements that 3-tesla will bring to orthopedic imaging, including better visualization of articular cartilage and all of the smaller joints, ligaments, and nerves in the body.
"There are a lot of injuries to the smaller ligaments of the fingers which are significant -- and many of them should be operated on, but it's hard to make a very specific reliable diagnosis right now by any technique," said Dr. John Crues of the RadNet Management group in Southern California.
As his group installs its first 3-tesla scanner in Tarzana, CA, Crues is also looking forward to better images in challenging areas like the labrum of the shoulder. "I think the added resolution one can get at 3-tesla, from what I've seen, will make it much easier to differentiate an anatomic variants from actual pathology," he said.
  |
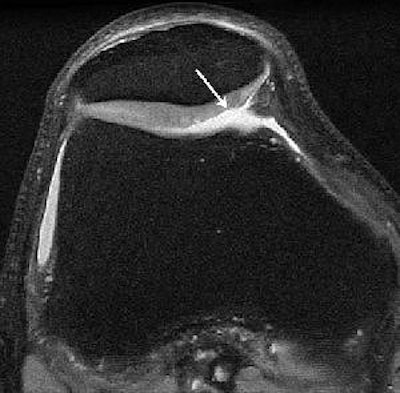
| Knee images in a 29-year-old man with knee pain. Axial proton-density image (TR/TE, 5,000/14; matrix, 512 x 384; slice thickness, 2 mm) acquired at 1.5-tesla shows fraying of lateral patella cartilage (arrow). Knee images in a 29-year-old man with knee pain. Axial proton-density image acquired at 3-tesla with identical parameters shows improved signal-to-noise ratio (SNR). Improved depiction of fraying of lateral patella cartilage (arrow) is seen at 3-tesla. Overall SNR at 3-tesla allows imaging at higher resolution. Gold GE, Suh B, Sawyer-Glover A, Beaulieu B, "Musculoskeletal MRI at 3.0 T: Initial Clinical Experience" (AJR 2004; 183:1479-1486). |
Referral advantage
Fueling the steady march from 1.5-tesla to 3-tesla in the U.S. is a combination of the interest in superior visualization and a competitive market for imaging that finds providers embracing any potential advantage. And 3-tesla MRI does offer competitive advantages.
"If you formulated the protocols well, you could scan your routine knees say twice as fast as the guy down the street, yet at the same time cater to a high-end orthopedic practice that's doing cartilage repair," said Dr. Garry Gold, an assistant professor of radiology at Stanford University Medical Center in Stanford, CA.
The six radiologists in Florida's NeuroSkeletal Imaging center are already sold on the advantages of 3-tesla MRI. The Melbourne, FL-based group has installed a 3-tesla scanner in each of its four outpatient imaging centers over the last two years.
"We've had a significant bump-up in the number of musculoskeletal MRIs being ordered, most likely as a result of the images provided by the 3-tesla scanner," said Dr. Thomas Magee, chief of musculoskeletal imaging for the group.
"What it's providing is very-high-resolution imaging, what we perceive as more accurate diagnoses," said Magee. "We're able to provide more definitive reports for the orthopedic surgeons and I think they appreciate that."
NeuroSkeletal Imaging has also sought to quantify the accuracy offered by 3-tesla imaging. In a study Magee presented at the 2004 RSNA meeting in Chicago, the group looked retrospectively 63 knee exams (fast spin-echo proton-density imaging at 2-mm slice thickness) where the patients subsequently underwent arthroscopy.
Arthroscopy confirmed the meniscal tears seen on imaging for all 63 patients and identified just two additional tears, giving 3-tesla MRI a sensitivity of 97% with 100% specificity. The most important aspect for surgeons and patients, Magee noted, "was that we didn't have any false-positive readings for meniscal tears."
Lagging developments
But others say that beyond improving diagnostic confidence, 3-tesla MRI as yet is only moving toward its ultimate potential.
"The advances in coil design at 1.5-tesla are so far ahead, currently, of the coil design at 3-tesla that the theoretical advantages of 3-tesla probably have not been fully realized," said Dr. William Palmer, director of musculoskeletal imaging at Massachusetts General Hospital in Boston.
"Even the coil selection at 3-tesla now is suboptimal," said Palmer, who was hoping to receive his first 3-tesla shoulder coil later this month. Still, he expressed enthusiasm about 3-tesla's future potential.
"With the newer coils, when they get developed at 3-tesla, we will be able to create comparable if not superior images in much less time," Palmer said. "I am confident that standard joint protocols -- no gadolinium, no contrast -- are going to be in the 15-minute range."
The faster scanning with 3-tesla is already providing challenges and opportunities for Palmer. For one thing, the computer program his group uses to schedule patients among nine available MRI scanners won't accept anything less than a 45-minute exam time. So the 3-tesla is instead taking on unscheduled patients.
"What we've guaranteed the orthopedists in our practice is if they have a same-day add-on request, we accommodate that," said Palmer. "The 3-tesla is very helpful because it does allow us to make protocol changes that shorten the time of imaging and allows us to squeeze these patients in and still get an excellent diagnostic study."
Due to the specifics of MR physics, Gold noted, 3-tesla actually provides a bigger mathematical gain in scan time than in resolution. "You can double the resolution at 3-tesla compared to 1.5, but you can go up to four times as fast," he said.
Cautionary notes
Shorter scan times are only one part of the protocol revisions that must occur when moving from 1.5- to 3-tesla MRI. Artifacts from metal fragments will be worse at 3-tesla, and chemical-shift artifacts at the interfaces of fat and water in the body must also be addressed.
The chemical-shift artifact, Palmer noted, "can create abnormalities when they don't exist, or it can make those abnormalities more difficult to see when they do exist. So the protocols need to be adjusted to minimize it. Not that it's that hard to do, but it requires another level of awareness -- it's another complexity to the system."
In addition, the increased energy deposition required for body imaging might limit 3-tesla in that application, observed Crues. And the safety of various aneurysm clips, spinal stimulators, and other items patients may have in their bodies is an obvious consideration.
"We still have a 1.5 available to scan some patients if there's anything questionable as to whether it can go on the 3-tesla," Magee said.
But while 3-tesla MRI may be an issue for some postsurgical patients, it offers exciting opportunities for surgery of the future, Gold said. "With the new methods of cartilage repair, we could maybe look and see whether the repair is integrating with the host cartilage, or the bone for that matter."
That's the kind of promise that counterbalances concerns about 3-tesla's impact on the economics of medicine, Crues said.
"I think it's highly likely that, with further experience at 3-tesla, we will find that it will have a significant positive impact upon diagnostic capabilities," Crues said. "And usually in musculoskeletal imaging, what that's meant is that it has fundamentally changed our understanding of pathology and has changed orthopedic management in ways that were never anticipated before."
By Tracie L. ThompsonAuntMinnie.com staff writer
February 22, 2005
Related Reading
The 3-tesla MRI swap: Why it's not a simple upgrade, January 27, 2005
High-field MR extremity systems: Is it time to be scared? November 17, 2004
NYU buys 7-tesla Siemens MRI, May 25, 2004
Low-field MR turns in varying results for MSK abnormalities, trauma, December 22, 2003
Four-tesla MRS tumor measurement cuts out unnecessary breast biopsies, November 25, 2003
Copyright © 2005 AuntMinnie.com


















